Renal Length (L), Width (W), the antero-posterior (AP) diameter, and volume (V). These are the measurement that you should take during a renal scan.
Other renal measurements are cortical thickness and parenchymal thickness.
In daily clinical practice, taking renal Length(L) and Width (W) is sufficient. You should always mention these measurements in your report.
Volume, cortical thickness, and parenchymal thickness are not measured in every patient. You should measure them only when there is a clinical indication, when you suspect any renal disease.
After reading this tutorial, you will be able to:
- measure renal length, width, and calculate volume
- measure parenchymal and cortical thickness
- normal measurement value
- know common pathologies, and
- common pitfalls and pearls.
Renal Length Measurement
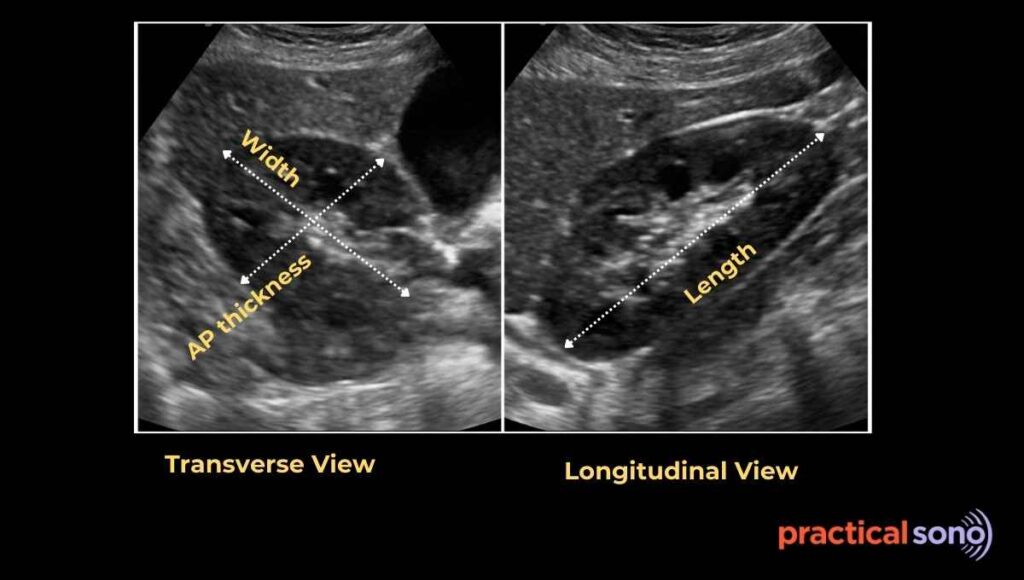
Renal length is the maximum distance from the upper pole to the lower pole of the kidney.
This is the single most important measurement. It best reflects the overall size of the kidney.
Now let’s understand how to measure it correctly:
- It is measured in the longitudinal view.
- Place the probe on the patient’s flank along the mid-axillary line.
- Keep the probe marker directed toward the head.
- Slowly adjust the probe until you get the kidney in its maximum length.
- Both the upper and lower poles must be clearly seen in the same image. (Rib shadow or bowel gas might obscure the view)
- Once you have the optimal image, place one caliper at the upper pole of the kidney and the second caliper at the lower pole.
- Always place the calipers on the renal capsule. Measure from capsule to capsule.

PracticalSono tips:
Remember, the kidney must be imaged in its true long axis. If you do not adjust the probe properly, you will not get a true longitudinal view. This can make the kidney look falsely small.
If you cannot see the kidney borders clearly, turn on tissue harmonic imaging. Harmonics make the borders sharper. This helps you identify the capsule clearly and place the calipers accurately.
Normal Kidney Length
In adult, normal renal length is approx. 9-12 cm.
Right kidney is smaller than left kidney. It is about 2 cm shorter. This is normal.
However, a difference of more than 2 cm between the two kidneys is considered abnormal.
Normal renal length in pediatric:
- Newborn (term): 4.0 – 4.5 cm
- 0–3 months: 4.5 – 5.5 cm
- 3–12 months: 5.5 – 6.5 cm
- 1–2 years: 6.0 – 7.0 cm
- 2–5 years: 6.5 – 8.0 cm
- 5–10 years: 8.0 – 9.5 cm
- 10–15 years: 9.0 – 11.0 cm
- ≥ 15 years: 9 – 12 cm
In children, both kidneys should be similar in size. Difference of more than 1 cm between right and left kidney is considered abnormal.
The left kidney is usually slightly longer than the right kidney. And, premature infants normally have smaller kidneys compared to term infants.
In case of children, height-based charts are more accurate than age-based charts, especially after infancy.
When evaluating kidney length in children, always correlate the measurement with the child’s age, height, and clinical context.
Large Kidney (Causes)
In adults, a kidney is considered enlarged when the renal length is more than 12 cm. Enlargement is also suspected when there is a clear size difference compared to the opposite kidney. A difference of more than 2 cm is abnormal.
Kidney width and thickness also help in assessment. A width significantly more than 4 to 6 cm or a thickness more than 3 to 5 cm suggests enlargement.
Renal volume is another important indicator. A volume greater than 190 mL in men or greater than 150 mL in women strongly suggests renomegaly.
Enlarged kidney diagnostic criteria
Length: >12cm (size difference of more than 2cm )
Width : > 4-6 cm
Renal Volume: > 190ml ( male) and >150ml (female)
Remember this. A kidney should never be labeled “enlarged” based on length alone without considering:
- Patient height and body habitus
- Age
- Pregnancy
- Hydration status
- Clinical scenario
The term “enlarged kidney” is more confidently used when increased length is accompanied by:
- Increased renal width and AP diameter
- Bulky appearance of kidney
- Preserved or increased parenchymal thickness
- Normal or mildly increased cortical thickness
Cause of Enlarged Kidney:
- Physiological
- Compensatory Hypertrophy
- Pregnancy
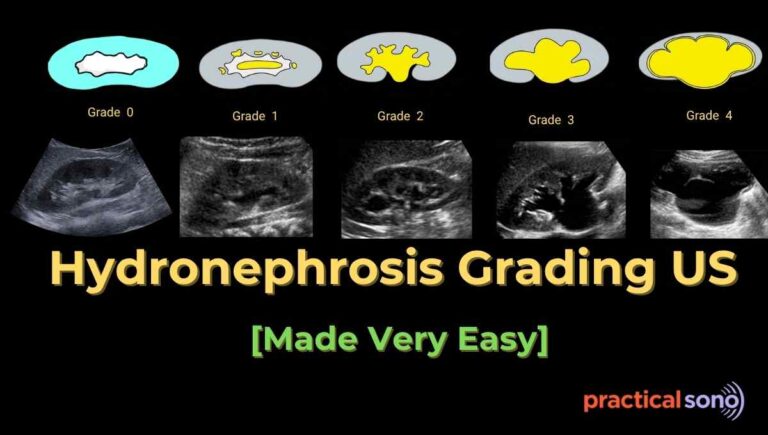
- Pathological
- Hydronephrosis
- Acute Pyelonephritis
- Acute glomerulonephritis
- Acute tubular necrosis
- Early diabetic nephropathy
- Polycystic Kidney disease
- Acute renal vein thrombosis
- Malignancy
Physiological Causes of Enlarged Kidney:
Compensatory hypertrophy occurs when one kidney is absent or not functioning properly. In this situation, the healthy kidney grows to handle the extra workload. It can increase up to one and a half times its normal size.
Pregnancy is another physiological cause. During pregnancy, it is common for the kidneys to increase in overall size. There may also be mild dilation of the collecting system due to normal hormonal and mechanical changes.
Small Kidney (Causes)
A kidney length of less than 8 cm suggests a small and shrunken kidney. This usually indicates chronic kidney disease with fibrosis.
Cause of Renal Atrophy/Shrunken Kidney:
- Congenital: Renal Hypoplasia, Renal Dysplasia
- Chronic Kidney disease
- Renal artery stenosis
- Chronic Pyelonephritis
- Reflux nephropathy
Enlarged Kidney: more than 12cm
Small Kidney: less than 8cm
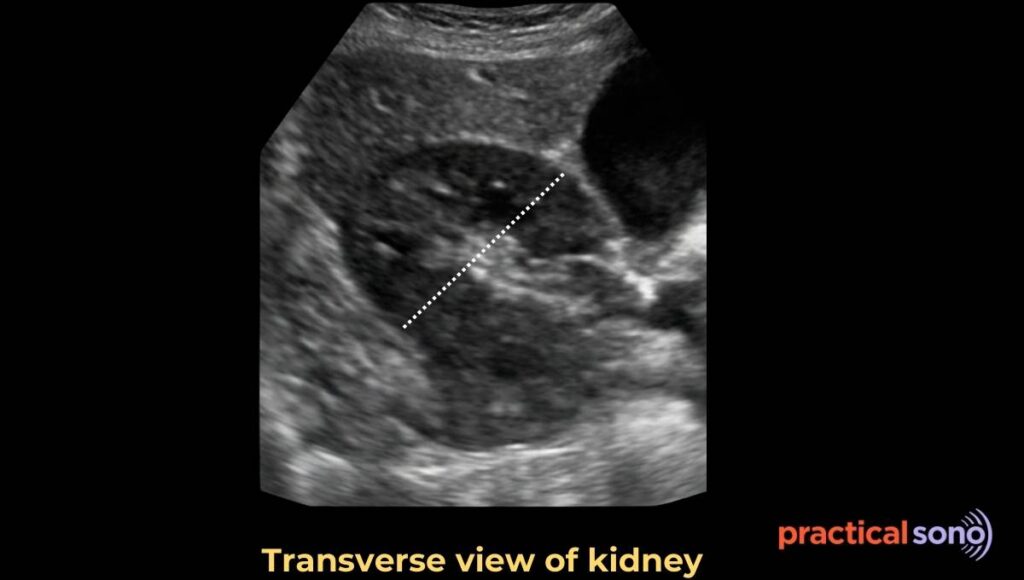
Renal Width Measurement
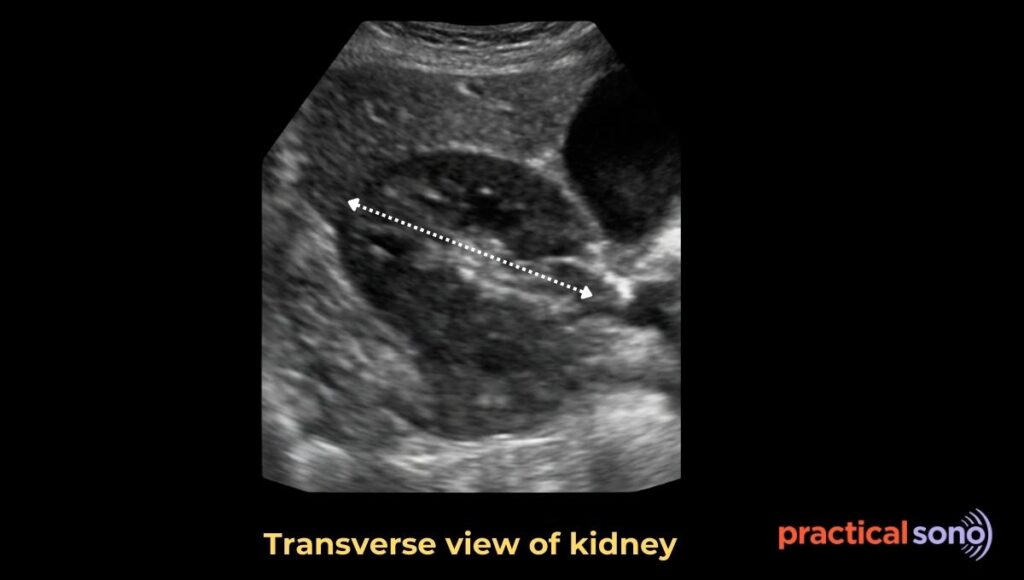
Renal width is the maximum transverse diameter of the kidney. It is measured in the transverse view at the level of the renal hilum.
To measure it correctly:
- First, get longitudinal view of kidney in mid axillary line and then rotate the probe anticlockwise. The probe marker should face downward toward the spine.
- Identify the widest part of the kidney, usually at hilum.
- Place the calipers from the outer edge of the medial cortex to the outer edge of the lateral cortex. Make sure the probe is perpendicular to the long axis of the kidney. This prevents underestimation of the width.
In adults, the average renal width is about 4 to 6 cm.
SonoPractical Tips:
You do not need to memorize this number. A simple rule is that the kidney width is usually about half of its length.
Kidney Width = Renal Length/ 2
Renal Anterior-Posterior (AP) thickness
Renal Antero-Posterior Thickness is the maximum anteroposterior dimension of the kidney. It is also measured in the transverse plane.
(QuickRevision: Renal width and AP diameter are measured in transverse view. Renal length is measured in longitudinal view.)
To measure it correctly:
- Get a true transverse section of the kidney, usually at the level of the renal hilum.
- The probe marker should face downward. (Towards spine)
- Measure from the anterior outer renal capsule to the posterior outer renal capsule.
- Take the measurement perpendicular to the renal width.
- Avoid oblique sections because they can falsely increase or decrease the AP diameter.
In adults, the average renal AP diameter is about 3 to 5 cm. AP thickness alone has limited value. It is mainly used to help estimate the overall renal size and calculate renal volume.
Renal Volume Measurement
Renal volume represents the overall size of the kidney. It correlates better with renal mass than any single linear measurement.
However, in routine adult renal ultrasound, renal volume is not measured regularly.
Renal volume reflects functional renal parenchymal mass more accurately than renal length alone.
Now let’s understand when renal volume should be measured.
Renal volume should be measured when a precise assessment of kidney size is clinically important.
- Renal transplant evaluation and follow-up.
- Useful in pediatric patients because volume correlates better with age and body surface area.
- In chronic kidney disease, renal volume helps when detailed documentation of renal mass is needed. I
- t is also measured in research studies or during serial follow-up when small size changes matter.
- Renal volume is important in congenital anomalies, dysplastic kidneys, and unilateral kidney disease to compare functional renal mass.
Now let’s see how renal volume is calculated.
Renal volume is calculated using the ellipsoid formula.
Renal volume = Length X width X AP diameter X 0.523.
You do not need to memorize this formula. It is already built into your ultrasound machine. To calculate renal volume, press the measure button and select kidney volume. (use kidney preset, if you don’t see this option) Then start taking the required measurements.
- First, measure the renal length in the true longitudinal plane from upper pole to lower pole.
- Next, measure the renal width in the transverse plane at the level of the renal hilum.
- Then measure the renal AP diameter in the same transverse plane.
Once all three measurements are completed, the machine will automatically calculate the renal volume.
Always calculate the volume of each kidney separately.
Normal adult renal volume is approximately:
Male: 120–200 ml per kidney
Female: 90–170 ml per kidney
Total combined renal volume is usually around 250–400 ml.
Reduced renal volume suggests
- chronic irreversible renal disease
- and, loss of nephron mass.
Enlarged renal volume may be seen in
- acute inflammatory conditions,
- obstruction,
- pregnancy, or
- early diabetic nephropathy.
Marked asymmetry in renal volume indicates chronic unilateral disease.
Renal Cortical Thickness Measurement
Renal cortical thickness is the distance from the outer renal capsule to the base of a medullary pyramid. It represents true cortical tissue, which contains most of the functioning nephrons.
Cortical thickness is measured in the longitudinal plane of the kidney.
Let’s understand how to measure it correctly.
- Obtain a clear longitudinal image showing a well-defined medullary pyramid.
- Place one caliper on the outer renal capsule. Place the second caliper at the base of the medullary pyramid, not at the tip.
- Measure perpendicular to the capsule.

Always take the measurement at the mid-pole of the kidney, where the cortex is best seen.
Avoid measuring over the renal columns or at the poles, as this can give inaccurate values.
In adults, the normal renal cortical thickness is about 6 to 10 mm. It may be slightly lower in elderly patients.
A cortical thickness of less than 6 mm suggests advanced chronic kidney disease.
Normal: 6-10mm
Abnormal: less than 6mm
Now let’s discuss when cortical thickness should be measured.
It should be measured when chronic kidney disease is suspected.
It is also important in ..
- medical renal disease,
- long-standing obstruction,
- reflux nephropathy,
- hypertensive nephropathy,
- and diabetic nephropathy.
Cortical thickness is useful during follow-up of patients with known chronic kidney disease.
Interpretation:
Reduced cortical thickness indicates chronic and irreversible renal damage and correlates with reduced renal function.
Cortical thinning is often a better marker of chronicity than renal length alone.
If cortical thickness is preserved but echogenicity is increased, this may suggest earlier stages of medical renal disease.
Cortical thickness should be reported when chronic kidney disease or medical renal disease is suspected.
SonoPractical Tips:
In normal kidneys with normal length and normal echogenicity, it is not necessary to mention cortical thickness.
Renal Parenchymal Thickness Measurement
Renal parenchymal thickness is the distance from the renal capsule to the renal sinus fat.
It represents the combined thickness of the renal cortex and medulla.
Measuring it helps assess the chronicity and severity of kidney disease, especially in obstructive conditions.
To measure it correctly:
- obtain a longitudinal image of the kidney through the mid-pole.
- Identify the bright echogenic renal sinus in the center.
- Place one caliper on the outer renal capsule and the second caliper on the outer margin of the renal sinus fat.
- Measure perpendicular to the capsule. Avoid measuring at the poles or over the columns of Bertin.

In adults, normal renal parenchymal thickness is about 15 to 20 mm.
Renal parenchymal thickness should be measured in cases of
- suspected chronic kidney disease,
- chronic or long-standing hydronephrosis,
- reflux nephropathy,
- follow-up of obstructive uropathy,
- evaluation of renal transplant function,
- or when renal length is borderline.
Reduced parenchymal thickness suggests chronic kidney damage and correlates with decreased renal function.
In obstructive uropathy, progressive thinning indicates chronic disease and poor recovery.
Preserved parenchymal thickness with pelvicalyceal dilatation usually favors acute obstruction.
Key Takeaway
Renal length and width are measured routinely during scan. Other measurement are taken only when indicated.
Always correlate with patient clinical history, body habitus, and age before interpreting the kidney size. As size alone won’t tell you much about the possible condition.
Hope you like this tutorial. Thank you for reading.