Uterus is not fixed. It can either bend forward or backward leading to different position within pelvis.
During pelvis scan, you should find the position of uterus and mention it on your report.
Why?
Mentioning the correct position of uterus will help clinicians to perform procedure like IUD insertion, dilation and curettage (D&C), and hysteroscopies without puncturing the uterine wall.
After reading this tutorial, you will:
- understand sonographic landmark around uterus
- learn how tilting and bending of uterus happens
- know the terminology and its meaning to correctly describe the position of uterus
- know the common uterine position and how to recognize them on ultrasound (both transvaginal and transabdominal)
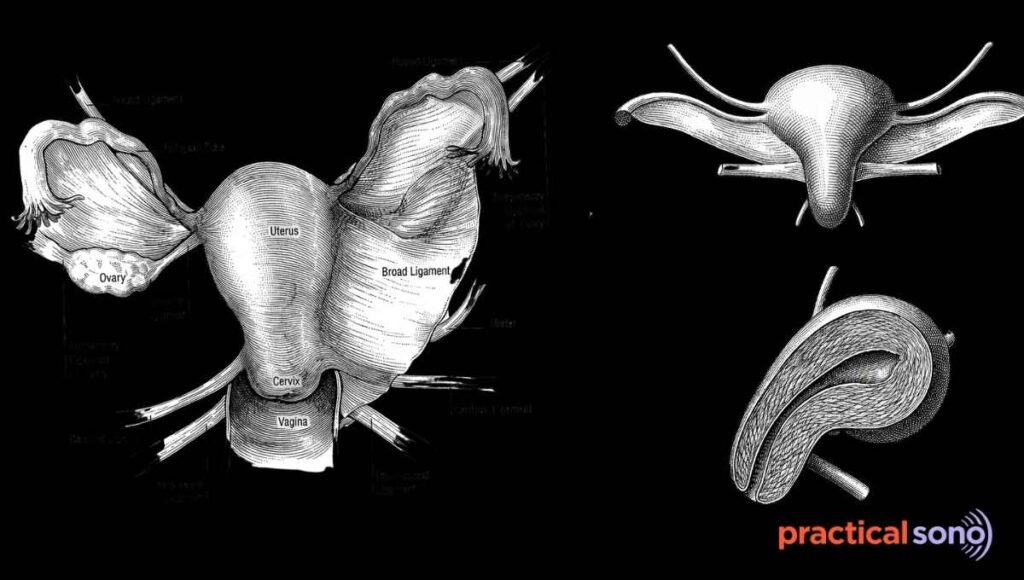
Basic Anatomy of the Uterus And Landmark
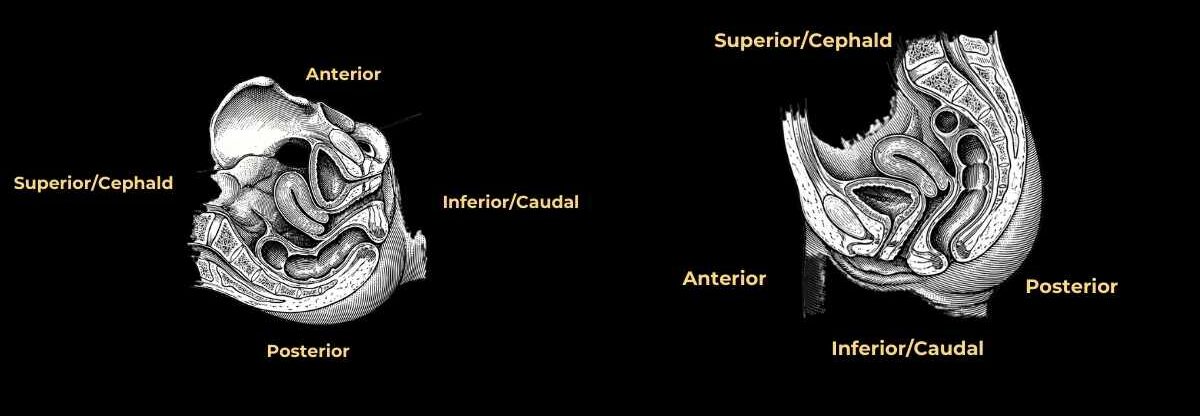
In the pelvis, the uterus lies in the midline.
Anterior to it is the urinary bladder, and posterior to it are the rectum and the spine. These anatomical relationships are extremely important when describing uterine orientation.
However, the uterus does not always stand straight. It may tilt forward toward the bladder or backward toward the rectum. This variation is normal and commonly encountered.
The uterus is divided into four main parts: the fundus, body, isthmus, and cervix.
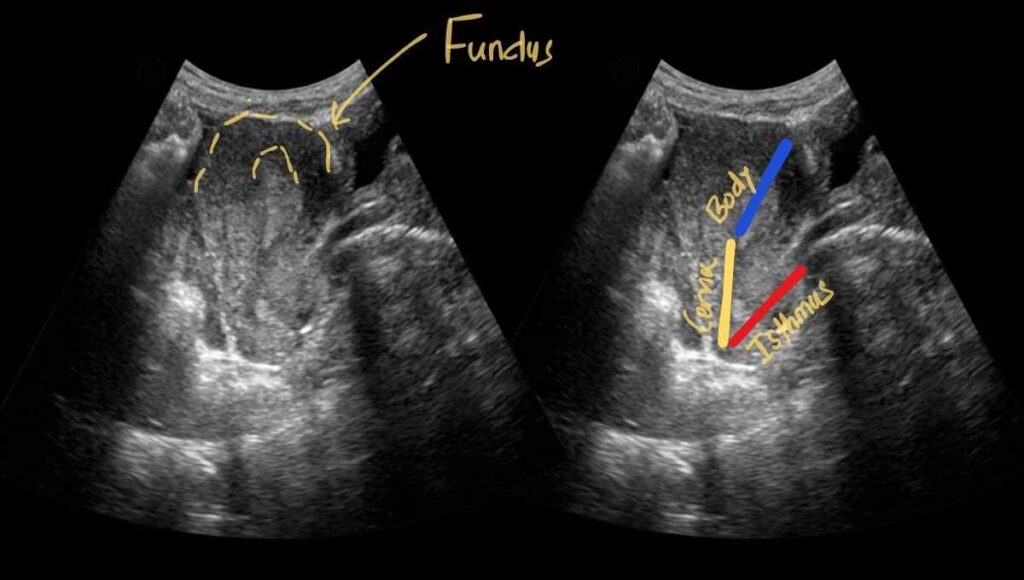
The fundus is the rounded uppermost portion. Below it lies the body, which forms the major central bulk of the uterus. The isthmus is a narrow transitional segment that connects the body to the cervix. The cervix forms the lower portion and opens into the vagina.
Understanding How the Uterus Tilts
To understand uterine position clearly, keep these structure in your mind: the vagina, the cervix, and the body of the uterus.
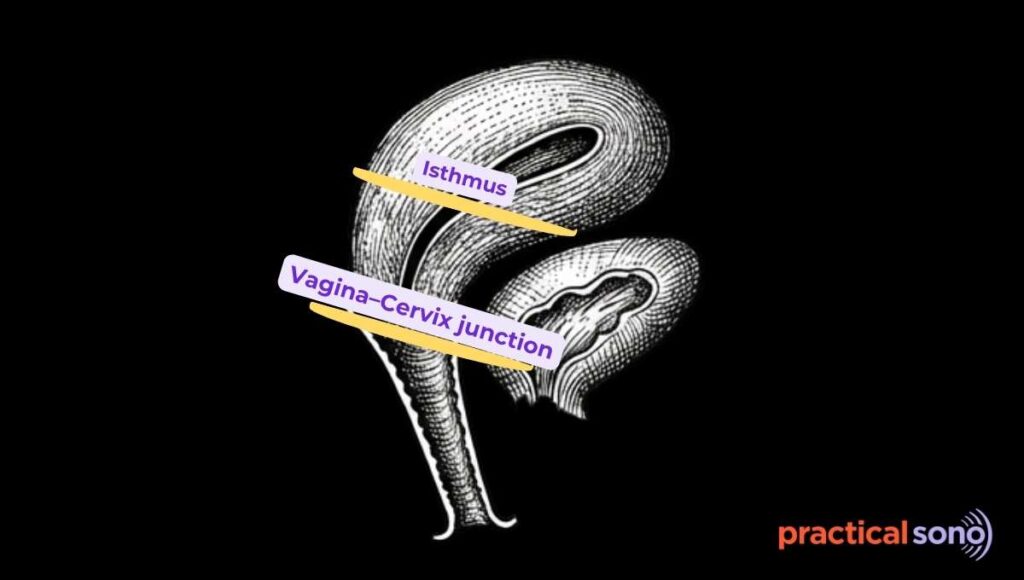
There are two key junctions where changes in direction occur.
- Vagina–Cervix junction
- Cervix–Body junction (Isthmus)
The uterus tilts and bends at these junctions.
The cervix tilts at its junction with the vagina. The body of the uterus bends at its junction with the cervix.
When describing the position of uterus, you should describe the position of cervix and body of uterus. They bend or tilt independently.
They might bend on same direction or in opposite direction.
Understanding Terminology to Describe Uterine Position
To describe uterine position correctly, you should know these terms: ante, retro, version, and flexion.
“Version” and “Flexion”
Version refers to the tilt of the cervix relative to the vagina. It describes the direction in which the cervix is pointing at the vaginal–cervical junction.
Flexion, on the other hand, refers to the bend of the uterine body relative to the cervix at the isthmus.
When describing uterine position, version is always mentioned first because it refers to the cervix. Flexion follows because it refers to the body of the uterus.
“Ante” and “Retro”
The terms ante and retro describe direction.
Ante means forward, meaning uterus is bend toward the bladder.
Retro means backward, meaning uterus is bend toward the rectum.
Because the bladder lies anterior to the uterus and the rectum lies posterior, these organs serve as reference points. ( important sonographic landmark)
PracticalSono Tips:
We describe these terminology assuming that patient is in standard upright anatomical position.
Even if a patient is lying supine in bed during scan, we still describe bladder as anterior and rectum as posterior. (Even though, bladder lies superior to uterus and rectum lies behind it.)
Common Uterine Positions
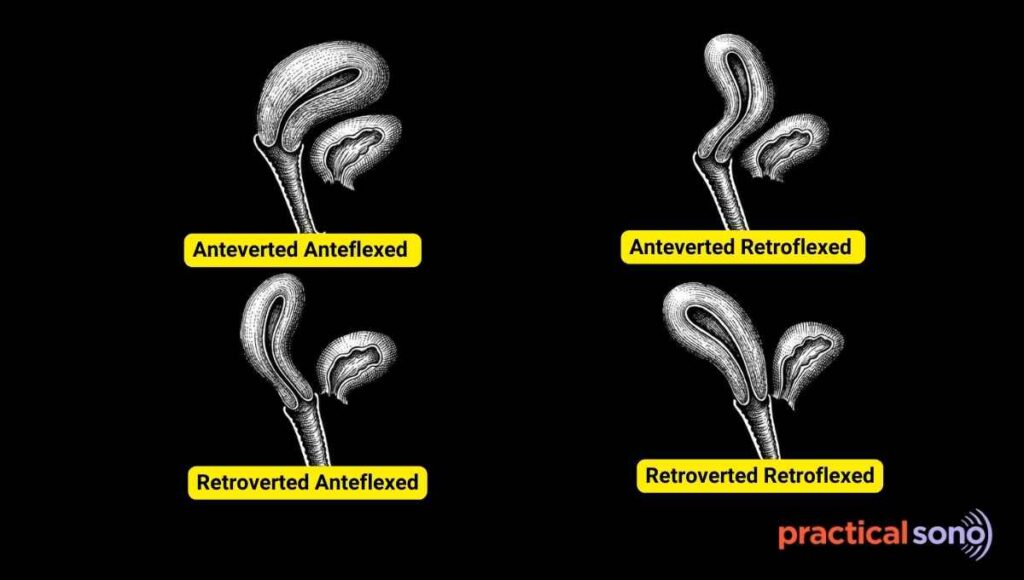
1. Anteverted Anteflexed (Common)
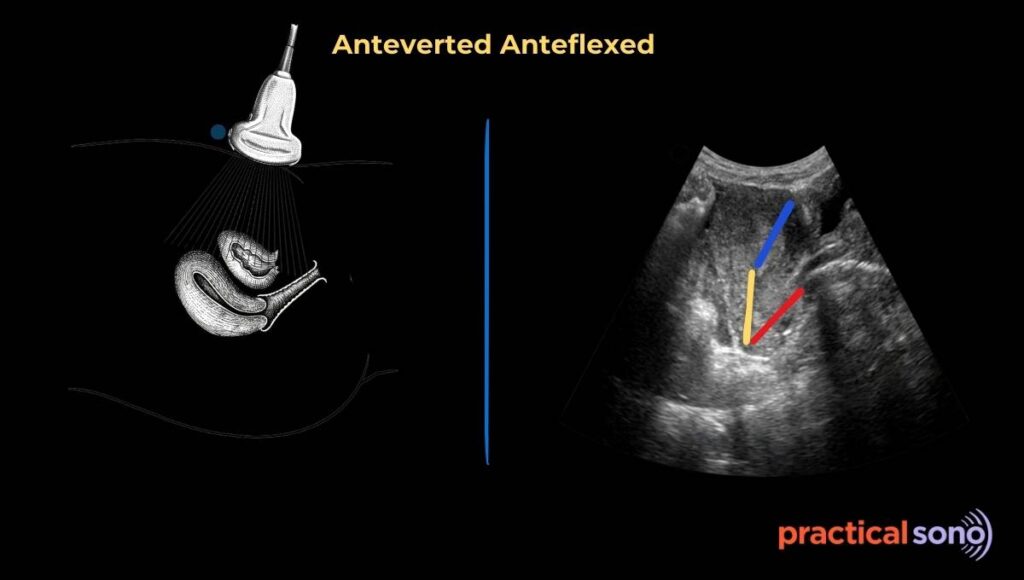
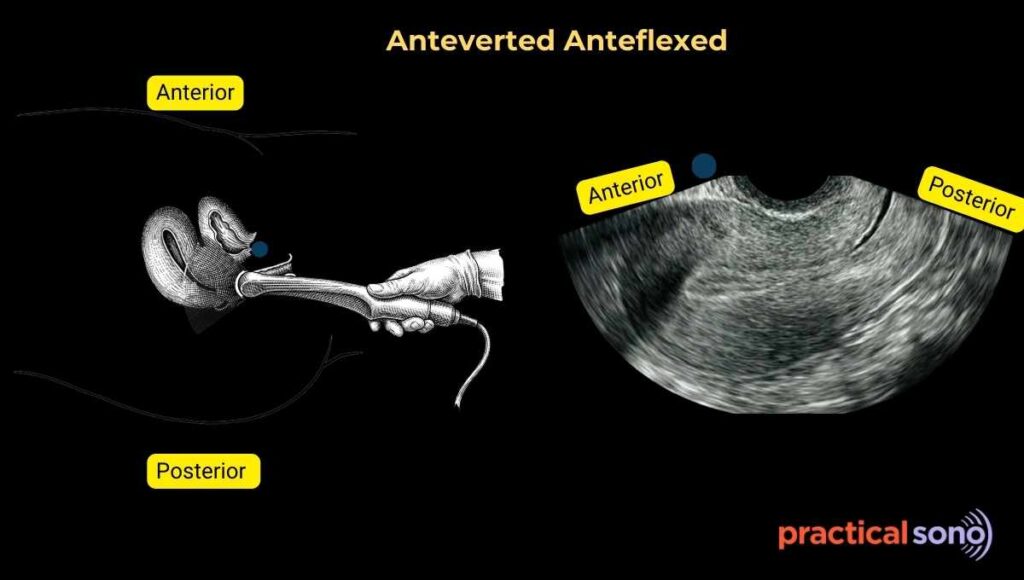
The most common uterine position is anteverted and anteflexed.
In this position, the cervix tilts toward the bladder and the body of the uterus also bends forward toward the bladder. This position is seen in approximately 70 to 80 percent of women and is considered the typical orientation.
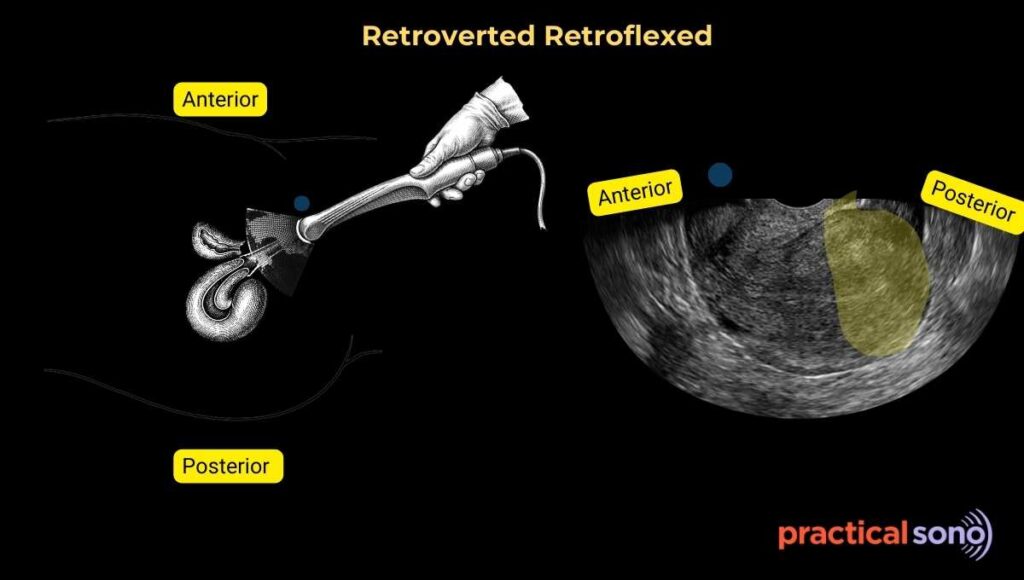
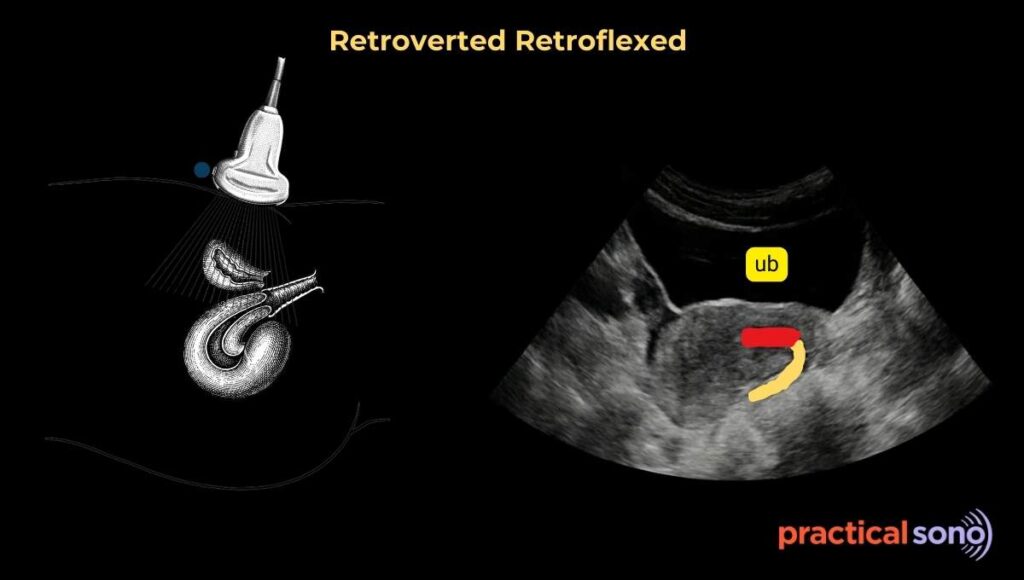
2. Retroverted Retroflexed
Another common variation is retroverted and retroflexed uterus. In this case, both the cervix and the uterine body are directed posteriorly toward the rectum. This position occurs in about 20 to 25 percent of women.
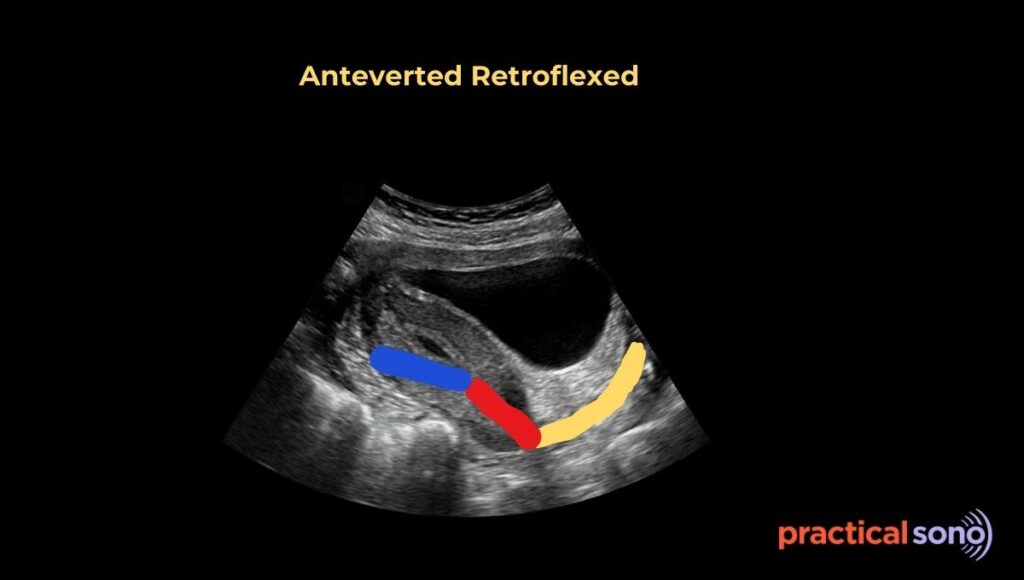
3. Anteverted Retroflexed
Less commonly, the cervix and body move in opposite directions. In an anteverted retroflexed uterus, the cervix tilts forward but the body bends backward.
4. Retroverted Anteflexed
In a retroverted anteflexed uterus, the cervix tilts backward while the body bends forward. These positions are uncommon and not frequently encountered in routine ultrasound practice.
5. Midline Uterus
In some women, the uterus may appear relatively straight without significant forward or backward tilt. This is referred to as a mid-position uterus.
It is important to emphasize that all of these positions are normal anatomical variations and do not by themselves indicate disease or infertility.
Influence of Bladder Filling on Uterus Position
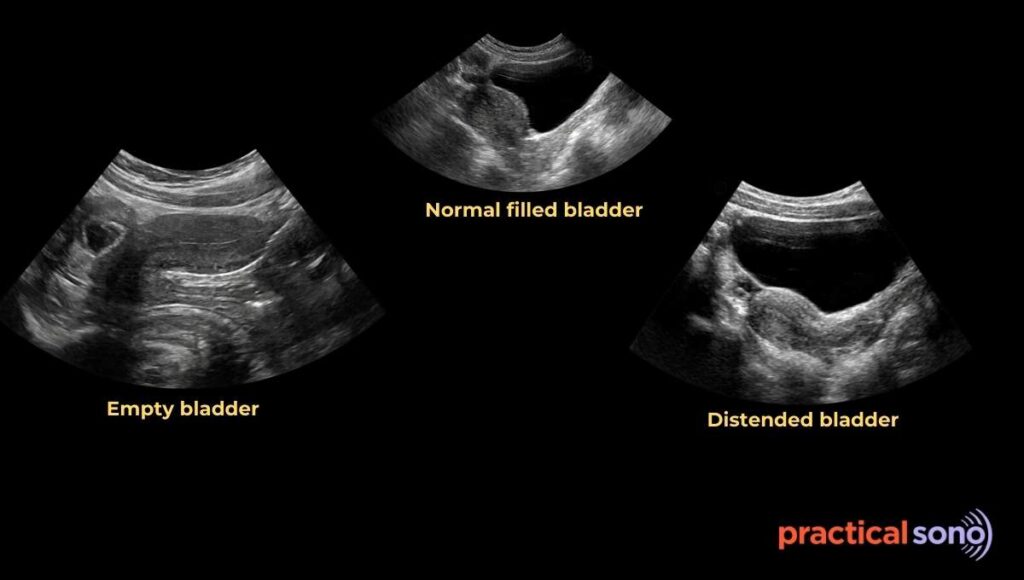
Bladder volume significantly affects the apparent position of the uterus, especially on transabdominal ultrasound.
When the bladder is comfortably filled, the uterus often appears moderately anteverted without extreme angulation.
When the bladder is empty, the uterus tends to fall forward, sometimes producing marked anteversion and anteflexion.
Conversely, if the bladder is overly distended, it can push the uterus posteriorly and mimic retroversion.
Understanding this relationship prevents misinterpretation during imaging.
Uterine Position in Transvaginal Ultrasound
In transvaginal scanning, the bladder is emptied, so it is not visible.
The probe marker is typically oriented upward at the 12 o’clock position, directed toward the anterior aspect of the patient’s body.
In a longitudinal view, if the fundus appears close to the probe marker on the anterior side of the image, the uterus is anteverted and anteflexed.
If the fundus appears away from the probe marker and directed posteriorly, the uterus is retroverted and retroflexed.
Important: Knowing the direction of probe marker is key to identifying the position of uterus during transvaginal scan.
Why the Uterus Changes Position
The uterus is a highly mobile organ supported by several ligaments, including the broad ligament, uterosacral ligament, and round ligament.
In most women, the natural tension of the round ligaments pulls the uterus forward over the bladder. This is the reason why anteverted anteflexed is the most common position.
In a smaller proportion of women, the uterus naturally tilts backward.
Pregnancy can significantly influence uterine position. During gestation, supporting ligaments stretch to accommodate the growing fetus.
After delivery, especially in multiparous women, these ligaments may not regain their original tightness. As a result, the uterus may assume a more mid-positioned or retroverted orientation.
Pathological conditions can also alter position. Scarring from endometriosis or pelvic inflammatory disease may pull the uterus into a fixed retroflexed position. Large fibroids can mechanically shift orientation.
An anterior wall fibroid may tilt the uterus forward, whereas a posterior wall fibroid may push it backward.
Uterine Position and Ovary Location
Normally, the ovaries lie lateral to the uterus within the ovarian fossa.
When the uterus is retroverted or retroflexed, the ovaries may appear more superolateral or deeper within the pelvis.
Because a retroverted uterus presses toward the rectum, the spatial relationship between uterus and ovaries can change.
This is particularly relevant during ultrasound evaluation.
Clinical Importance of Knowing Uterine Position
Although variations in uterine position are usually normal, knowing the orientation is clinically important.
It guides safe insertion of intrauterine devices, helps prevent perforation during endometrial biopsy, and assists in planning dilation and curettage procedures.
Understanding uterine direction ensures that instruments are advanced in the correct anatomical plane, minimizing pain and complications.
Key Takeaway
In summary, uterine position is described by assessing the tilt of the cervix (version) and the bend of the uterine body (flexion).
“Ante” indicates direction toward the bladder, and “retro” indicates direction toward the rectum.
Most women have an anteverted anteflexed uterus, but variations are common and usually normal. Mastering these concepts is fundamental for accurate ultrasound interpretation and safe gynecologic practice.