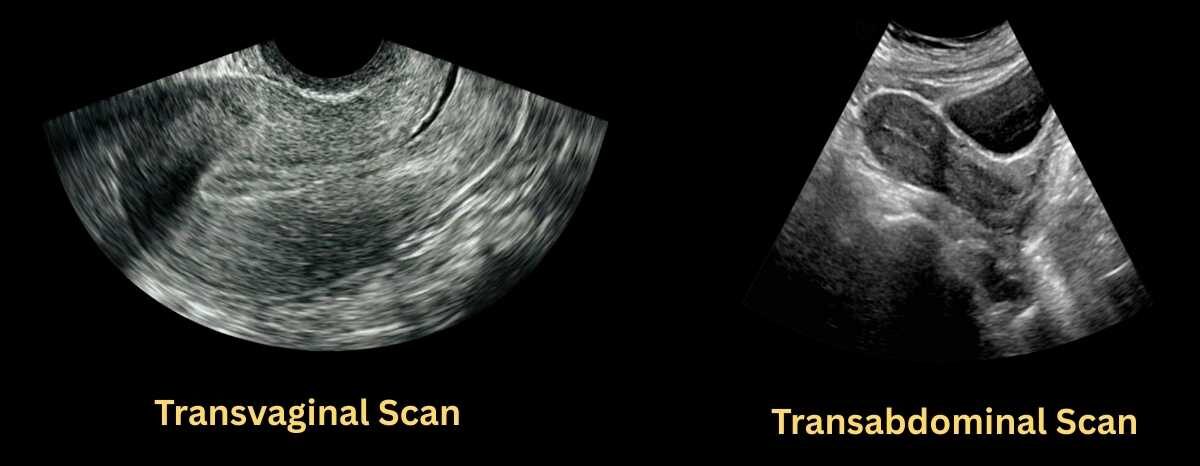
For endometrial thickness measurement, transvaginal ultrasound (TVS) is always preferred over transabdominal ultrasound (TAS). Because it provides higher resolution and a clearer image of the endometrium.
In fact, endometrial thickness should be interpreted on transvaginal ultrasound only.
After reading this tutorial, you will
- understand normal sonographic anatomy of endometrium and its layers
- know the changes in endometrium layers during different menstrual phase
- know standard protocol to measure the thickness of endometrium on Transvaginal and Transabdominal scan
- know the interpretation of endometrium thickness in premenopausal and post-menopausal woman
- Know how endometrium appears in different age group
- understand common pathologies that increases the endometrium thickness.
Endometrium Layers and Ultrasound Appearance
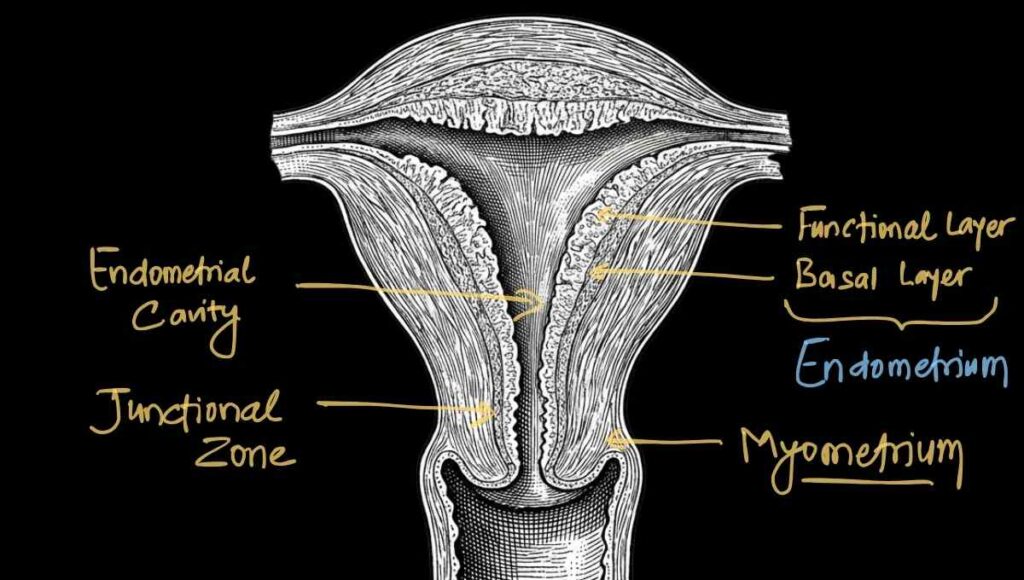
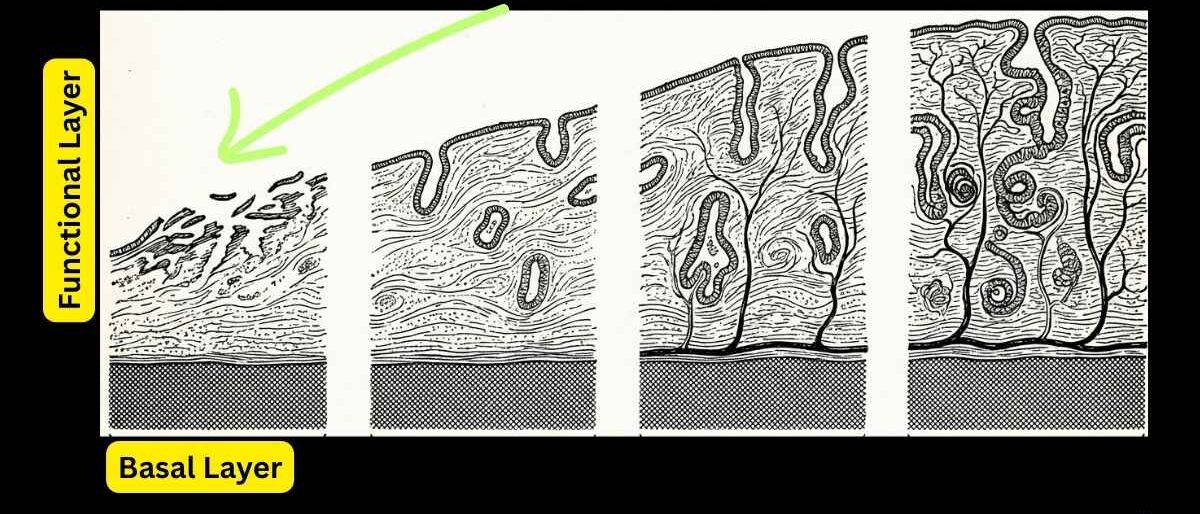
The endometrium has two layers:
- superficial functional layer
- deep basal layer
The functional layer responds to hormones. Its thickness changes during the menstrual cycle. This is the layer that sheds during menstruation if pregnancy does not occur.
The deep basal layer remains intact. It acts as the foundation for regeneration of the endometrium.
The junctional zone is the innermost layer of the myometrium. It lies directly in contact with the endometrium.
Endometrial cavity is potential space where the anterior and posterior walls normally touch each other. In a non-pregnant state, the cavity is collapsed. It only becomes a true cavity when distended by blood or fluid.
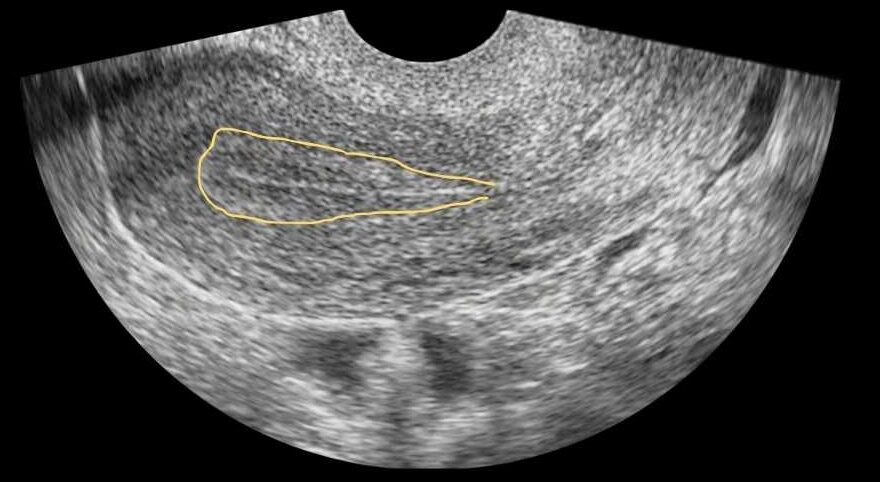
On ultrasound, the endometrium is seen as a central echogenic line, also called an echogenic stripe.
It is surrounded by a hypoechoic layer and then an outer hyperechoic layer.
- Thin Central bright line :The thin bright line in the center is formed by the interface between the two opposing endometrial walls. This represents the endometrial canal.
- Hypoechoic Middle Layer: The hypoechoic middle layers represent the functional layer. This appears as a thicker, darker area. It changes in size during the menstrual cycle. It looks like a dark band surrounding the central bright line. It appears hypoechoic due to edema and glands.
- Outer basal layer: The outer basal layers appear hyperechoic.
- Junctional halo: The junctional halo is also called the subendometrial halo. It represents the junction between the endometrium and the myometrium. It appears as a thin, dark, hypoechoic halo surrounding the brighter echogenic endometrium.
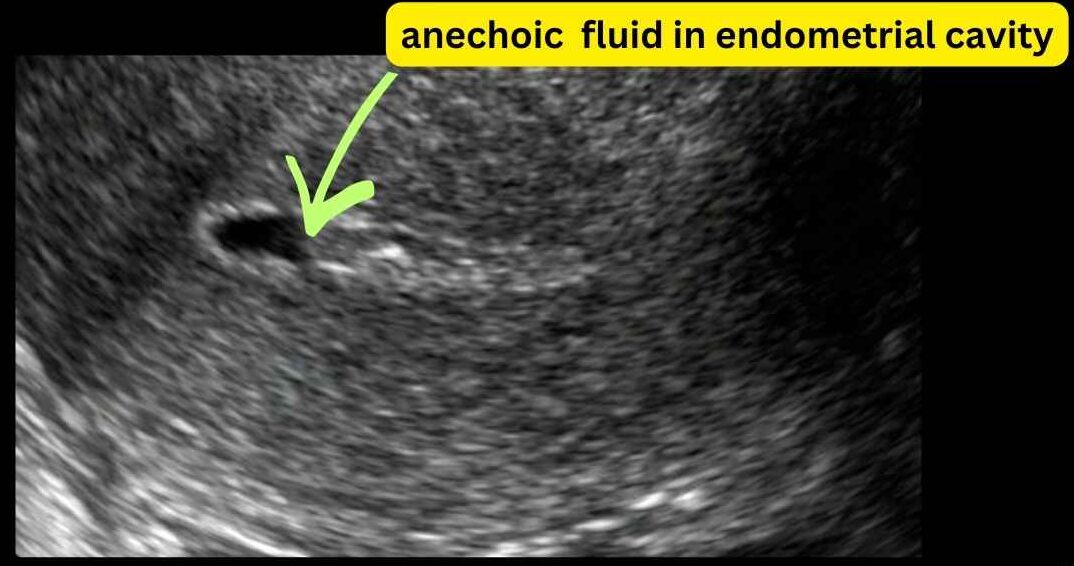
- If the endometrial cavity is filled with fluid, you will not see the bright central echogenic line. Instead, you will see a dark anechoic endometrial cavity.
Standard Method to Measure Endometrial Thickness
Transvaginal ultrasound is the gold standard for measurement of endometrial thickness. This is because it provides better resolution of the endometrial lining.
- Measurements must be taken in the midsagittal or longitudinal plane of uterus.
- The entire length of the endometrium should be visible. This includes the area from the fundus to the endo cervical canal. You must look at the whole endometrium, not just one part.
- The endometrium must be visualized completely by sweeping from side to side. A single static image is not enough. Focal pathology, such as early adenocarcinoma, can be missed if you do not examine the entire endometrium. Do not accept indistinct margins.
- The hypoechoic inner myometrium, called the junctional halo, must be excluded from the measurement.
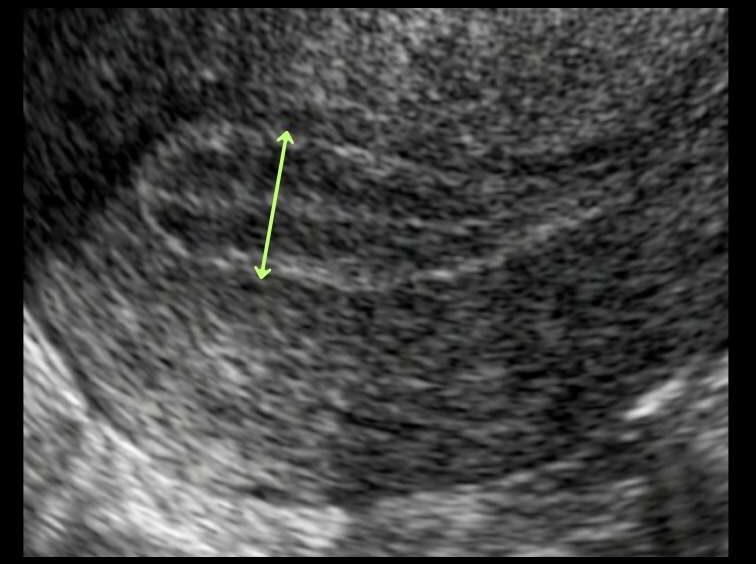
- Measure the maximum anterior-posterior diameter at the thickest part of the endometrium. This is usually in the fundal region.
- The measurement must be taken perpendicular to the long axis of the uterus.
- Place the calipers at the thickest portion of the endometrial echo.
- Measure from one basal endometrial interface to the other across the canal. Measure from echogenic border to echogenic border.
- Your measurement should include both the anterior and posterior layers.
- Do not include any fluid, myometrium, intra cavitary clot, mass, or polyp in the measurement.
- If fluid is present in the cavity, measure each endometrial wall separately. Then add the two measurements together.
- If the entire endometrium cannot be visualized, report it as not well seen.
In about 5 to 10 percent of cases, the endometrium cannot be adequately visualized. This may be due to fibroids, obesity, or uterine position.
In these cases, do not measure it blindly.
Clearly state in your report that the endometrium is not well visualized. If you’re suspecting any pathology, saline infusion sonography may help in better visualization of endometrium.
However, in postmenopausal women with bleeding and a poorly visualized endometrium, endometrial biopsy is usually the next step.
Transabdominal Ultrasound and Endometrium
Transabdominal ultrasound is not ideal for measuring endometrial thickness due to lower resolution image. It is less reliable and may overestimate or underestimate thickness.
Instead of thickness, focus on the appearance of the endometrium.
- Assess whether the endometrial lining is homogeneous or heterogeneous.
- Look for a thin, bright central line endometrial stipe. A distorted or absent midline echo may suggest a polyp or a fibroid.
- Check whether the junctional halo is smooth and regular. Irregular, interrupted, or speculated sub endometrial halo suggests: malignancy, polyp, and adenomyosis.
- Look for any fluid in the endometrial cavity.
- Identify rounded bright masses, which may represent polyps.
- Also. look for darker, well-defined masses. These may be submucosal fibroids protruding into the cavity.
If the endometrium poorly defined or appears abnormal in a symptomatic patient, recommend further evaluation.
This may include transvaginal ultrasound, saline infusion sonography, or endometrial biopsy.
And, always remember to correlate the ultrasound appearance with the patient’s menstrual phase or menopausal status.
Endometrium Thickness Change during Menstruation Cycle
In menstruating woman, the endometrium changes its thickness and appearance throughout the menstrual cycle.
This change happens in superficial functional layers only. This is the layer that shed during menstruation. The deep basal layers remain intact.
The menstrual cycle is divided into four phases:
- Menstruation/bleeding phase
- Early proliferative
- Late proliferative
- Secretory phase
The proliferative phase before ovulation is driven by estrogen. Progesterone maintains the endometrium during the secretory phase after ovulation.
The endometrium is thinnest during menstruation phase and thickest during the secretory phase.
#1 Menstruation/bleeding phase
During menstruation, the endometrium measures about 2 to 4 millimeters.
It appears irregular with mixed echogenicity due to blood and clots.
Small fluid can be normal.
#2 Early proliferative phase
During the early proliferative phase, the endometrium appears thin and organized with a bright central line.
Thickness is about 4 to 6 millimeters.
This is the best phase to evaluate small polyps or focal lesions.
#3 Late proliferative or pre-ovulatory phase
During the late proliferative or pre-ovulatory phase, the endometrium shows a tri laminar or triple-line appearance.
Thickness can reach about 10 millimeters.
The triple-line appearance is a normal estrogen-driven fertile lining.
It consists of an
- outer hyperechoic basalis,
- middle hypoechoic functional layer,
- central echogenic stripe formed by the interface of the opposing endometrial walls.
#4 Secretory phase
During the secretory phase, the endometrium becomes thick, uniform, and echogenic.
Thickness is usually 7 to 14 millimeters and can reach up to 16 to 20 millimeters.
PracticalSono Tips:
There is no universally accepted upper limit of thickness of endometrium in this phase. A 24 mm endometrial thickness in secretory phase in reproductive age woman can be normal.
Small endometrial cyst and folds are normal in this page. Endometrial folds may mimic polyps, so caution is needed.
Interpreting endometrium can be misleading, especially in this phase
If abnormal bleeding is present, and you’re suspecting any abnormalities, a follow-up ultrasound in the early proliferative phase is always recommended before diagnosing polyps or abnormal thickness.
PracticalSono Tips:
The early proliferative phase, from day 5 to 9, is the best time to evaluate the endometrium. The lining is thin, making small lesions easier to detect.
Endometrium Appearance at Different Ages
Appearance of endometrium change in different age group. This, you should keep in your mind while looking at endometrium.
Neonatal Endometrium:
The neonatal uterus is temporarily prominent due to maternal hormone influence.
It is visible on ultrasound in about 97 percent of infants during the first week of life.
It appears as a bright echogenic central line. Small amounts of clear fluid in the cavity are common and normal. This occurs due to hormone withdrawal after birth.
Prepubertal Endometrium
As maternal hormones decline, the uterus enters a quiet, infantile state until about 7 or 8 years of age.
The endometrium becomes very thin and is often difficult to see on a standard scan. It usually measures less than 1 millimeter.
In infants aged 4 to 12 months, the lining is visible in only about 50 percent of girls.
As a girl approaches puberty, the lining may begin to thicken slightly, reaching around 2 millimeters before the first period.
Postmenopausal Endometrium
After menopause, low estrogen causes the endometrium to become inactive and undergo atrophy.
It appears as a smooth, thin, uniformly bright line. The thickness is less than 5mm.
Women on hormone replacement therapy may have a slightly thicker lining, usually between 8 and 11 mm.
Interpretation of Endometrial Thickness in Premenopausal woman
In menstruating women, there is no single cut-off value for thickness of endometrium.
Ask her last menstruation period. (LMP). LMP will give you idea about her menstrual phase, so that you can anticipate the change in endometrium during that period.
Interpret your finding based on phase of her menstruation cycle, symptoms, general appearance of endometrium.
Ask these questions yourself when evaluating the endometrium in a menstruating woman.
- Does the endometrial size match the phase of menstruation? Always correlate thickness with the menstrual phase.
- Is the patient symptomatic? If she has abnormal uterine bleeding, endometrial thickness becomes more important and further evaluation may be needed.
PracticalSono Tips:
Always correlate the last menstrual period with the thickness of the endometrium. If the patient has vaginal bleeding, the thickness becomes more important.
Next, look at echogenicity and echotexture of endometrium. Look for focal mass, polyp, cyst, and fluid in endometrial cavity.
Check whether the endometrium is heterogeneous or irregular. An irregular and heterogeneous endometrium is highly suggestive of carcinoma.
Look for disruption of the junctional halo. This can be seen in adenomyosis or invasion by endometrial carcinoma.
Assess for any polyps, fibroids, or cystic lesions.
Look for fluid in the endometrial cavity. Fluid and debris may be seen in endometritis. However, fluid can also be seen during the menstruation phase, so always correlate clinically.
Finally, look for any change in the vascularity of the endometrium.
If you suspect pathology, repeat the scan in the early proliferative phase. This is usually between days 5 and 9 of the menstrual cycle.
Also, you can recommend saline infusion sonography (SIS) or endometrial biopsy based on your clinical correlation.
Interpretation of Endometrial Thickness in Premenopausal woman
In postmenopausal women, the endometrium is normally thin, usually less than 5 millimeters, and homogeneously hyperechoic.
Always ask if the patient has postmenopausal bleeding. Any postmenopausal bleeding is high risk for carcinoma and requires careful evaluation.
What is Postmenopausal bleeding?
“Postmenopausal bleeding is defined as any vaginal bleeding in a postmenopausal woman, except expected cyclic bleeding with sequential hormone therapy.”
In postmenopausal woman, 4mm commonly used as cutoff.
Endometrial thickness is more than 4mm and patient is having Per vaginal bleeding, consider high risk and advise biopsy, even if the endometrium appears homogeneous.
If it is 4mm or less, it does not require biopsy. Keep patient on regular follow up to see change in endometrial thickness.
Remember, if there is
- Heterogeneous echotexture or irregular margins
- Endometrial fluid
- Focal polyp lesion
- Persistent vaginal bleeding
- Increasing endometrial thickness on follow up scan
In these condition, biopsy is advised regardless of thickness of endometrium.
In postmenopausal women without bleeding, the risk of cancer is very low. Endometrial thickness of 5 millimeters or less is usually normal.
Thickness between 5 and 8 millimeters is commonly benign and can be observed unless suspicious features are present.
Thickness greater than 11 millimeters often warrants biopsy even if the patient is asymptomatic.
Endometrial cancer usually causes bleeding early. And, to avoid unnecessary biopsies, a higher thickness threshold is kept in asymptomatic.
Hormone Replacement therapy
Hormone replacement therapy (HRT) can alter the endometrium.
Because of this, the endometrium may appear thicker than in naturally postmenopausal women.
In this group also, bleeding status is more important than thickness alone.
Even if patient is on hormone replacement therapy, if she is having per vaginal bleeding
And her endometrial thickness is 4 millimeters or more, it requires evaluation.
The 4 mm cutoff still applies to women on HRT. Because cancer can occur in a lining between 5 and 8 mm. If the patient is not bleeding, the situation is different.
There is no universally fixed cutoff in this group, but clinical consensus provides guidance.
Most experts accept that an endometrial thickness up to 8 millimeters can be physiologically normal in women on HRT.
Values more than 8 mm deserve individualized judgment; more than 11 mm usually warrants evaluation.
The risk of malignancy is very low if the endometrium looks smooth and homogeneous. There should be no focal lesions, no fluid in the cavity, and the margins should be regular.
If you suspect any endometrial pathology during ultrasound, always recommend further evaluation. This may include endometrial biopsy, hysteroscopy, or saline infusion sonography.
Tamoxifen, which is used in mainly breast cancer treatment, can cause cystic thickening of endometrium and polyp. In this case also, there is no cut-off value. If there is bleeding, biopsy is required regardless of thickness.
Causes of Endometrial Thickening
Let us talk about why the endometrium becomes thick.
Physiological :
The endometrium is normally thick in the late menstrual cycle. It is also thick in early pregnancy. Peri-implantation changes can also make the endometrium appear thick.
Hormonal:
Hormone replacement therapy can increase endometrial thickness. Tamoxifen can cause stromal hypertrophy. It can also cause cystic endometrial changes and polyps. Unopposed estrogen exposure increases endometrial thickness. This is seen in anovulatory cycles, such as in PCOS. Obesity can also increase estrogen levels. Estrogen therapy is another cause.
Pregnancy-related causes:
Retained products of conception can cause endometrial thickening. Subinvolution of the placental site is another important cause.
Endometrial pathology:
These include endometrial hyperplasia. Endometrial polyps can also thicken the endometrium. Endometrial carcinoma is an important and serious cause.
Inflammatory causes should not be missed. Endometritis can lead to a thickened endometrium.
Structural causes:
Intrauterine adhesions with trapped blood can cause thickening. Cervical stenosis can cause hematometra.
In this case, the endometrium appears distended. Obstruction of the uterine or vaginal outlet can also occur. This leads to hydrometra, hematometra, or pyometra.
Endometrium Not Well Visualized
Transvaginal ultrasound is recommended for proper endometrial evaluation. It gives better detail and accuracy.
But, sometimes the endometrium is poorly visualized.
This can happen due to fibroids. Adenomyosis can also obscure the view. Scars inside the uterus may interfere. Blood or pus within the cavity can also reduce visualization.
Marked obesity or abnormal position of uterus also cause poor visualization of endometrium.
Endometrial thickness can be decreased with long-term Oral contraceptive pill use. Thinned out endometrium can be difficult to visualize in ultrasound.
However, in many postmenopausal women, a very thin endometrium is normal. An invisible endometrium can also be normal if there is no vaginal bleeding.
Calcified endometrial stripes are commonly seen in old premenopausal woman. They are usually benign and not a cause for concern.
If the endometrium is not visualized, always mention this in the report. Recommend further evaluation when clinically required.
Key Takeaway
The endometrium is a dynamic structure. It changes with age and with the phase of the menstrual cycle.
Always measure the endometrium at its thickest point, usually near the fundus.
The measurement should be perpendicular to the uterine axis.
Include both the anterior and posterior walls of the endometrium.
Exclude the junctional halo.
Do not include endometrial cavity fluid, clot, or mass.
If fluid is present in the cavity, measure both endometrial walls separately and add the two measurements.
In menstruating women, endometrium size changes throughout the cycle.
There is no exact cutoff for pathology.
The endometrium can reach 20 millimeters or more in the secretory phase and still be normal.
Instead of focusing on numbers, evaluate echogenicity, echotexture, fluid in the cavity, cysts, local masses, polyps, or any irregularity or break in the junctional zone.
In postmenopausal women, bleeding is high risk for cancer.
If bleeding is present and thickness is greater than 4 millimeters, further evaluation and biopsy may be needed.
Even without bleeding, heterogeneous or irregular endometrium, fluid in the cavity, breaks in the junctional zone, or focal masses require further evaluation.
The endometrium is not always visualized.
If it cannot be seen, do not comment on its thickness, report it as not well visualized.
Always correlate your findings with the patient’s symptoms and menstrual cycle phase.