When you say liver size, it usually means craniocaudal diameter of the right lobe of the liver. It should be measured in mid clavicular line.
This is standard technique that you should follow.
After reading this tutorial, you will:
- learn to measure the size of liver
- know normal and abnormal liver size according to age
- diagnostic criteria for hepatomegaly
- know the common hepatomegaly mimicker (Hepatomegaly vs Riedel’s Lobe)
Why measure the right lobe?
The right lobe is chosen because it is much larger than the left lobe. It is about five to six times bigger, so it better represents the overall liver size.
Changes in liver size are easier to detect in the right lobe.
The right lobe also has clear anatomical landmarks.
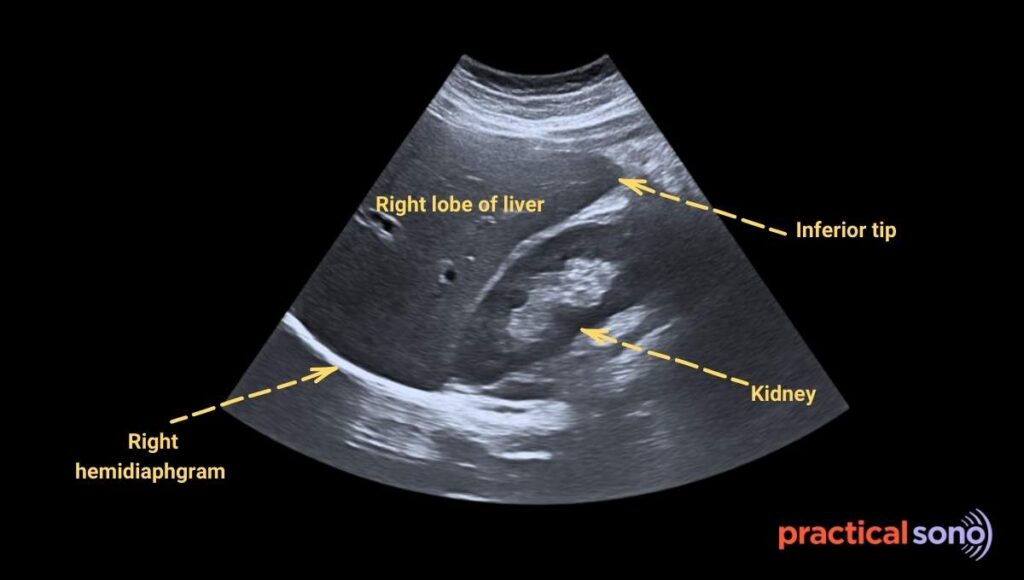
- The right hemidiaphragm
- and the inferior tip.
These landmarks can be visualized well in a single longitudinal view.
The left lobe has an irregular shape and is harder to measure accurately.
Why measure at midclavicular line?
The midclavicular line is an imaginary vertical line drawn from the midpoint of the collarbone.
It is used as a standard reference for measuring liver length.
Measuring at the midclavicular line ensures consistency.
This allows different sonographers to measure the liver at the same location every time.
Measurement of Liver size/Cranio-Caudal (CC) Length of Liver
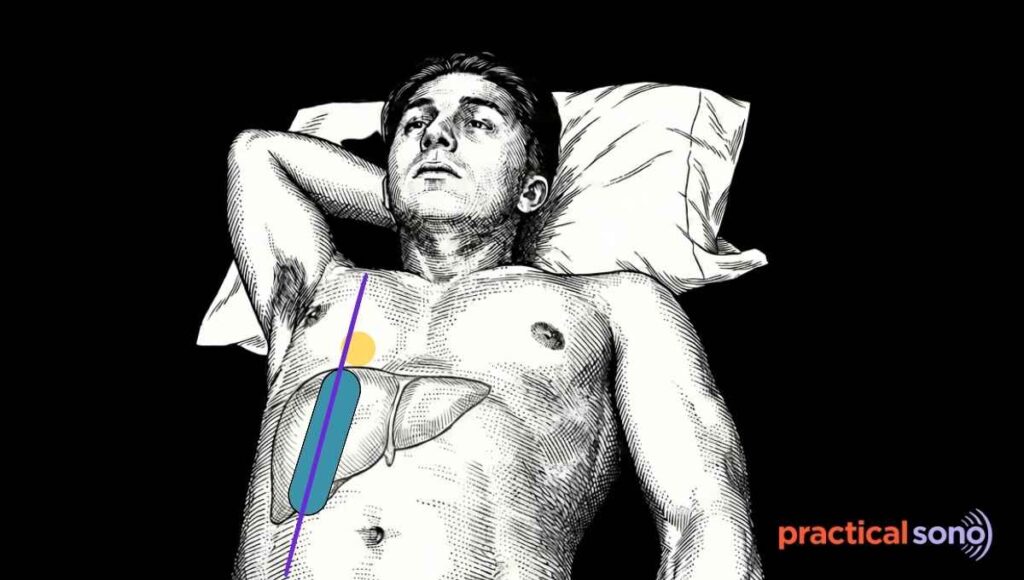
- Position: The patient should lie in a supine position, flat on their back.
- Ask the patient to raise the right arm above the head. This widens the intercostal spaces. It helps you see the liver dome more clearly.
- Use a low frequency curvilinear probe. This probe gives good penetration and a wide field of view.
- Place the probe in a longitudinal, or sagittal, orientation. Align the probe exactly along the right midclavicular line. Correct alignment is essential for accurate liver length measurement.
- Ask patient to take deep breath and hold. Always take measurements during a deep inspiratory breath-hold. Deep inspiration pushes the liver downward. This makes the diaphragm and the inferior tip of the liver easier to see on the screen.
- Once the liver is visualized in the sagittal plane at the midclavicular line, begin by identifying key landmarks.
- First, identify the diaphragm. It appears as a bright, curved echogenic line at the top of the image.
- Next, visualize the inferior tip of the right lobe of the liver.
SonoPractical Tips:
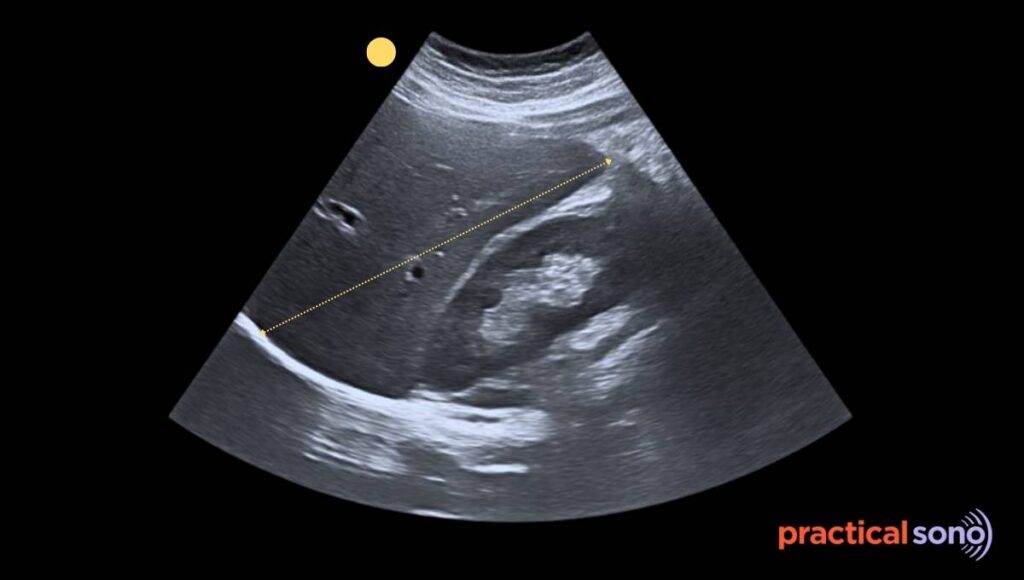
Make sure the entire liver, from the dome to the tip, is included in one image. You may need to gently rock the probe to achieve this view.
- Measure the craniocaudal length in a straight vertical line. Start from the dome of the liver just below the diaphragm..
- Place the caliper them from outer margin to outer margin, capsule to capsule. Do not measure in an oblique or angled plane.
The measurement must be taken in a true sagittal plane.
Sometimes, the ultrasound window is too narrow.
You may not see both the diaphragmatic surface and the inferior tip on the screen at the same time.
In this situation, estimate as accurately as possible where the unseen edge would end.
Place your calipers based on your best anatomical judgment.
Normal Liver Size
Liver size increases with height and body surface area and decreases with age.
| Age Group | Normal Range (MCL) | Typical Average |
| Newborn (0–1 month) | 5.0 – 6.5 cm | 5.7 cm |
| Infant (1–12 months) | 6.5 – 8.0 cm | 7.5 cm |
| Child (1–5 years) | 7.5 – 10.0 cm | 8.8 cm |
| School Age (6–12 years) | 9.0 – 12.5 cm | 11.0 cm |
| Adolescent (13–18 years) | 10.0 – 14.5 cm | 13.5 cm |
| Adult Female | 12.0 – 14.5 cm | 13.5 cm |
| Adult Male | 13.5 – 15.5 cm | 14.5 cm |
Hepatomegaly
A liver span >16 cm is widely accepted as hepatomegaly.
Measurements between 15.5 cm and 16.0 cm are often considered “borderline enlarged” and are interpreted based on the patient’s body size.
Hepatomegaly Criteria in Pediatric
| Age Group | Upper Limit (95th Percentile) |
| Newborn (0–3 months) | > 8.0 – 8.5 cm |
| Infant (6–12 months) | > 9.5 – 10.0 cm |
| Child (2–6 years) | > 11.0 – 12.0 cm |
| School Age (8–12 years) | > 12.5 – 13.0 cm |
| Adolescent (14–16 years) | > 13.5 – 14.0 cm |
Diagnose Hepatomegaly without Measuring (Tricks)
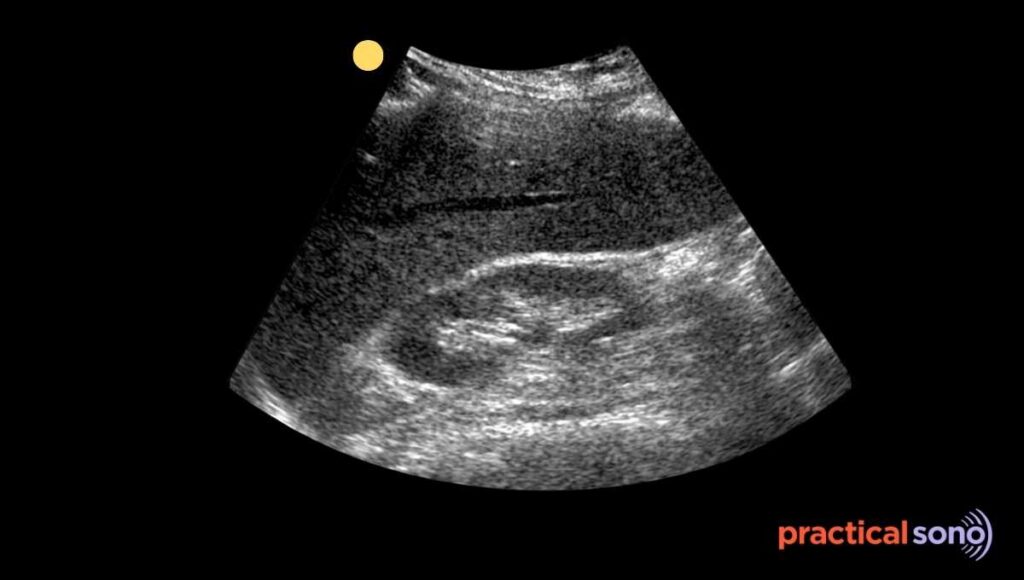
When liver size increases, inferior tip of the liver goes beyond the lower pole of kidney.
This eyeballing technique can tell you whether liver is enlarged or nor without measuring it.
Normally, the right lobe does not extend much beyond the lower pole of the right kidney. It usually ends around halfway down the kidney.
If the liver extends clearly below this level, hepatomegaly should be suspected.
A normal liver has a sharp and pointed inferior border.
If the edge looks rounded or blunted, it often indicates liver swelling.
Eyeballing technique: Inferior tip of liver beyond the lower pole of right kidney –> probably large liver (think of heptomegaly )

Cause of Hepatomegaly
- Fatty Liver/ Metabolic dysfunction-associated steatotic liver disease
- Alcohol-Related Liver Disease (ALD)
- Infections and Inflammation: viral hepatitis, infectious mononucleosis, liver abscess
- Storage disorder : glycogen storage disease, hemochromatosis , wilson’s disease
- Primary Liver Cancer: Hepatocellular carcinoma or cholangiocarcinoma.
- Metastatic Cancer: Most common malignant cause; cancer spreading from the colon, breast, or lung
- Congestive hepatopathy (right sided heart failure, budd-chiari syndrome
- Toxic and Drug-Induced Injury
- Medication Overdose: Common with acetaminophen (Tylenol).
- Herbal Supplements: Certain products like kava, black cohosh, and valerian root are linked to liver injury.
Riedel’s Lobe: Mimicker of Hepatomegaly
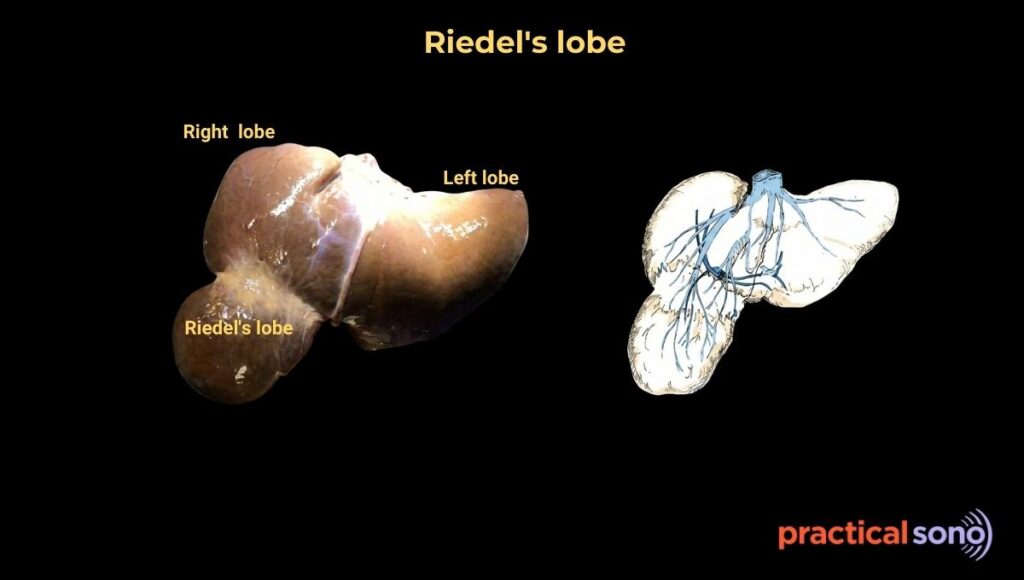
Riedel’s lobe is a common normal anatomical variant.
It appears as a tongue like downward projection of the right lobe of the liver.
Because it extends inferiorly, it can mimic hepatomegaly.
It is not a true accessory lobe. It is simply a shape variation of the existing right lobe.
Riedel’s lobe is much more common in females. Female to male ratio: 3:1 It is seen in about 3.3 percent to 31 percent of the population.
The exact cause is debated.
It may be congenital due to abnormal development of the hepatic bud. It may also be acquired. Chronic inflammation or traction from gallbladder disease may play a role.
On ultrasound, Riedel’s lobe is often mistaken for hepatomegaly or an abdominal mass.
To differentiate it from true liver disease, look for key features.
- The inferior edge remains sharp and pointed unlike true hepatomegaly, where the edge is rounded or blunted.
- Echotexture: The echotexture of Riedel’s lobe is normal. It looks identical to the rest of the liver parenchyma.

- Here, the left lobe is usually normal in size. However, in true hepatomegaly, the entire liver is typically enlarged.
Why you should know this?
Clinically, Riedel’s lobe may be felt as a mass in the right lower abdomen.
This can lead to unnecessary investigations if it is not recognized.
In rare cases, the lobe can twist on itself, causing acute abdominal pain.
It may also cause mild discomfort by pressing on nearby organs such as the stomach or kidney.
Key Takeaway
Measurement of liver size usually means taking the craniocaudal diameter of the right lobe of the liver in mid-clavicular line.
Liver size more than 16cm is hepatomegaly. You can gauges the size of liver by looking at the inferior tip of the liver. In hepatomegaly, tips usually passes the lower pole of right kidney.