Mesenteric lymphadenitis is frequently seen in children and young adult. It is a common mimicker of acute appendicitis.
After reading this tutorial, you’ll will
- anatomy of mesentery lymph node and its type
- understand how normal lymph node appears on ultrasound
- understand the difference between retroperitoneal and mesenteric lymph node
- know the diagnostic criteria for mesenteric adenitis on ultrasound
- know how to report your finding
Anatomy of Mesenteric Lymph Node
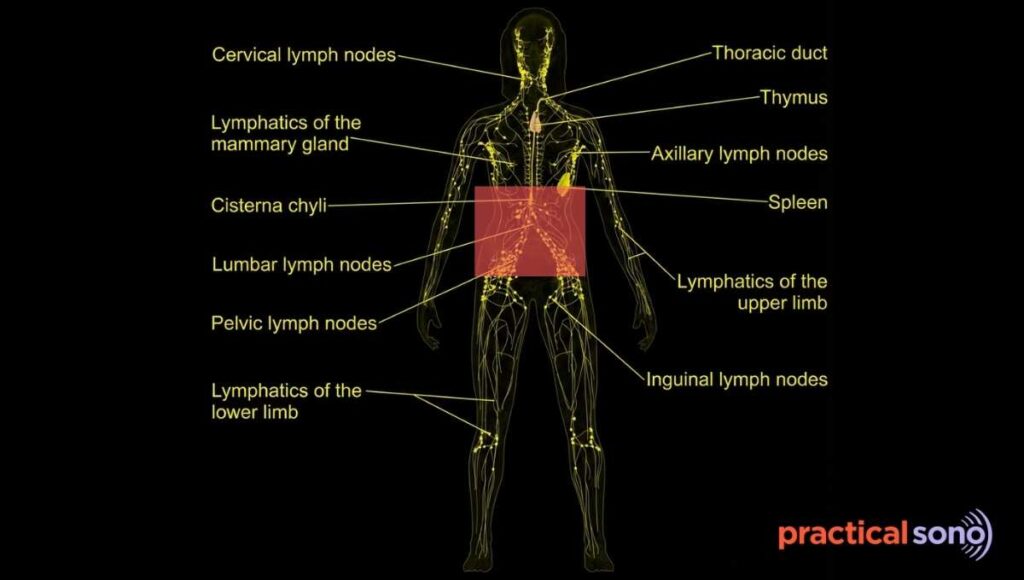
Mesenteric lymph nodes are an important part of the abdominal lymphatic system. They help drain lymph from the intestines and surrounding structures.
These lymph nodes are divided into groups based on their location.
- Superior mesenteric lymph node
- Inferior mesenteric lymph node
Superior Mesenteric Lymph Node
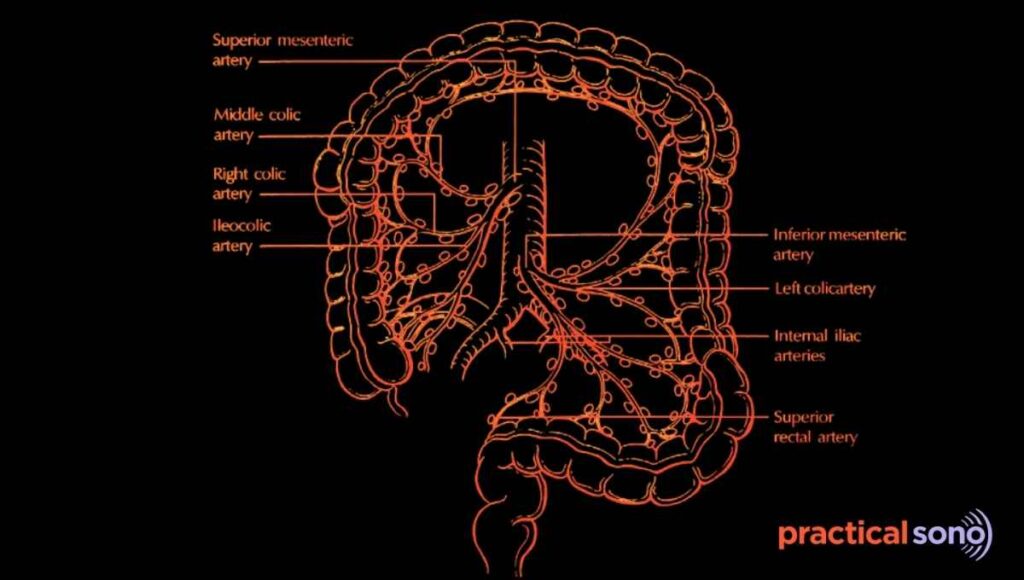
The superior mesenteric lymph nodes form a large group. There are about 100 to 150 nodes in this group. They drain the midgut. The midgut includes structures from the duodenojejunal flexure to the mid transverse colon.
- Juxtaintestinal mesenteric nodes are located very close to the wall of the small intestine. They lie along the peripheral arterial arcades.
- Intermediate mesenteric nodes are found along the jejunal and ileal arteries.
- Central superior mesenteric nodes are located at the root of the superior mesenteric artery.
- The ileocolic and mesocolic nodes drain the cecum, appendix, ascending colon, and transverse colon.
Lymph flows from the intestinal wall to the juxtaintestinal nodes. It then passes to the intermediate nodes and then to the central superior mesenteric nodes.
From there, lymph enters the intestinal lymphatic trunk and finally drains into the cisterna chyli.
Inferior Mesenteric Lymph Node
The inferior mesenteric lymph nodes form a smaller group. This group usually contains about 8 to 10 nodes. They drain the hindgut.
The hindgut includes the distal transverse colon, descending colon, sigmoid colon, and proximal rectum.
- Left colic nodes drain the descending colon.
- Sigmoid nodes are located within the sigmoid mesocolon.
- Superior anorectal or pararectal nodes are found close to the rectum.
Lymph from the inferior mesenteric nodes usually flows to the superior mesenteric nodes or directly to the preaortic nodes near the origin of the inferior mesenteric artery.
Appearance of Normal Mesenteric Lymph Node on Ultrasound
Mesenteric lymph nodes are most commonly seen in the right lower quadrant and around the umbilical region.
When you scan these areas using a high frequency linear probe, you may see images like this.
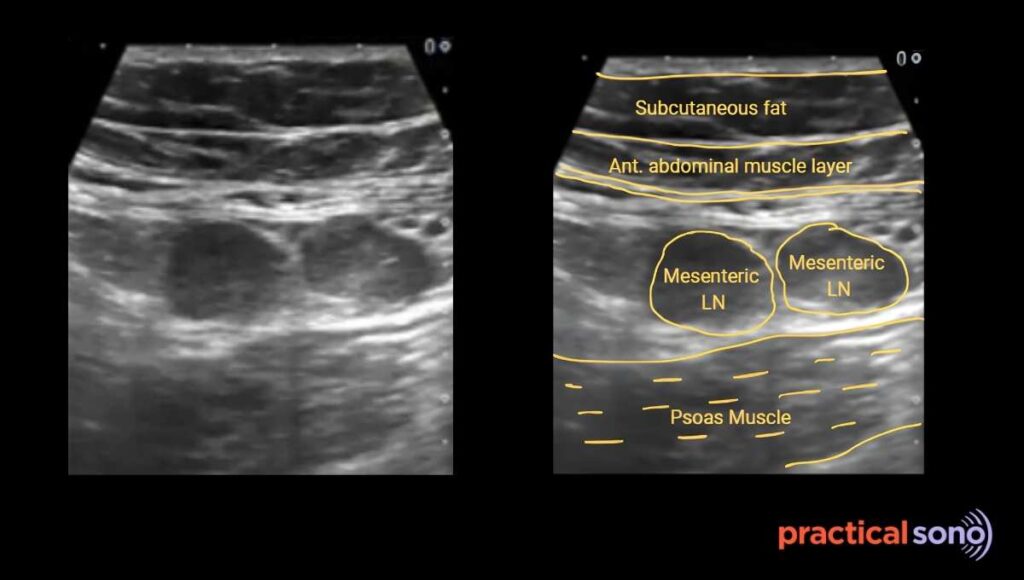
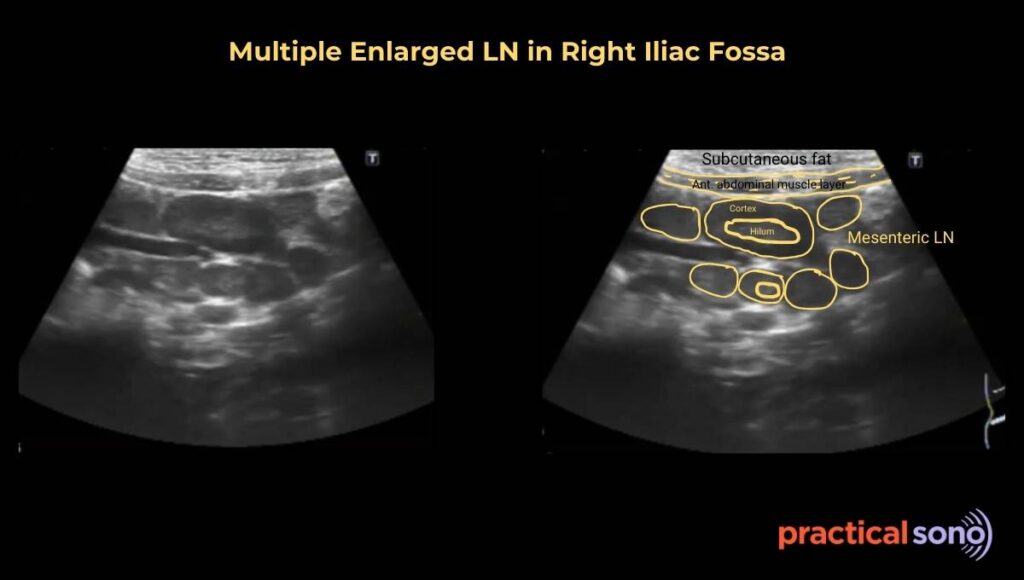
This is a longitudinal view of a mesenteric lymph node in the right iliac fossa.
This is the most common site for enlarged or reactive mesenteric lymph nodes. They are often located in front of the right psoas muscle. These nodes are usually seen in clusters.
They are commonly found near the terminal ileum and the cecal region. This is especially true in cases of mesenteric adenitis.
In the right lower quadrant, the psoas muscle is a very reliable posterior landmark. Enlarged lymph nodes are usually seen just anterior to it.
If bowel gas is blocking your view, do not get frustrated. Apply gentle graded compression. You can also place the patient in the left lateral decubitus position. This helps move bowel loops and improves the acoustic window.
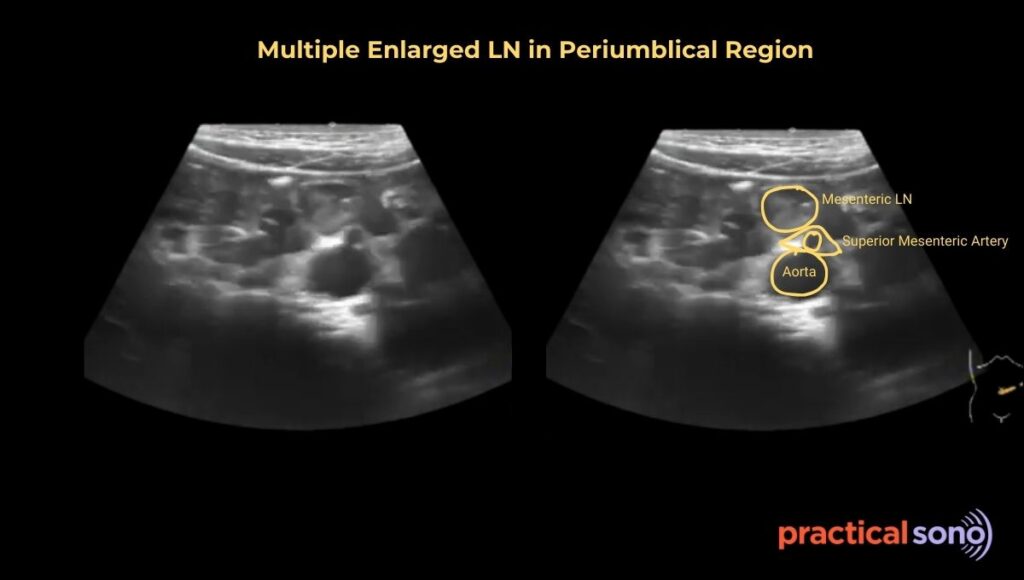
The periumbilical region is a high yield area for finding mesenteric lymph nodes. This area lies over the root of the mesentery, where the largest number of lymph nodes are present.
The lymph nodes in this region are mainly clustered around the Superior Mesenteric Artery and the Superior Mesenteric Vein.
They are usually seen within the bright echogenic fat of the mesentery. They lie between the anterior abdominal wall and the deeper retroperitoneal structures, such as the aorta.
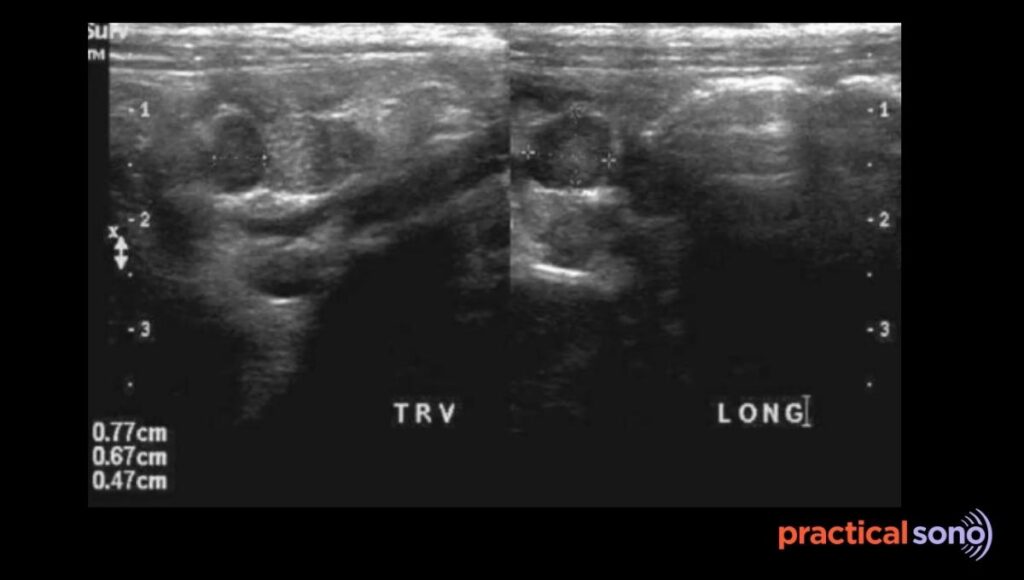
On ultrasound, they usually appear oval or kidney bean shaped. They are hypoechoic, which means they look darker than the surrounding fat.
In the center, you will often see a bright echogenic hilum. This is the part where blood vessels enter the node.
These nodes are often seen in chains or clusters. They follow the branching pattern of the mesenteric vessels.
Use a high frequency linear probe for better detail because these nodes are relatively superficial. Apply steady and gentle pressure with the probe.
This helps push away gas filled small bowel loops that may hide the mesenteric root.
Use color Doppler to identify central hilar blood flow. This helps you confirm that the structure is a lymph node and not a small bowel loop or a fecalith.
Retroperitoneal vs Mesenteric Lymphadenopathy on Ultrasound
Mesenteric and retroperitoneal lymph nodes are different based on their position, mobility, and drainage.
Understanding these differences helps you avoid wrong interpretation on ultrasound.
Location:
Mesenteric lymph nodes are pre aortic. This means they lie in front of the aorta. They are mainly clustered around the origins of the superior mesenteric artery and the inferior mesenteric artery.
Retroperitoneal lymph nodes are located deeper. While a few may be pre aortic, most are found beside or behind major vessels.
Para aortic nodes lie to the left of the aorta. Para caval nodes lie to the right of the inferior vena cava. Interaorticocaval nodes lie between the aorta and the inferior vena cava. If you see lymph nodes lateral to or behind the aorta, they are retroperitoneal.
Mobility:
Mobility is another important clue. Mesenteric lymph nodes lie within the folds of the mesentery. Because of this, they are relatively mobile. When you apply gentle pressure with the probe, these nodes may shift slightly.
Retroperitoneal lymph nodes are fixed. They are attached to the posterior abdominal wall. When you apply compression with the transducer, these nodes do not move.
Drainage Pattern:
Drainage pattern also gives you important clinical clues. Mesenteric lymph nodes mainly drain the gastrointestinal tract. They are commonly enlarged in inflammatory bowel conditions and in mesenteric adenitis.
Retroperitoneal lymph nodes, especially para aortic nodes, drain the urogenital system. This includes the kidneys, testes, and ovaries. These nodes are often the first site of metastasis in cancers arising from these organs.
Both mesenteric and retroperitoneal lymph nodes are usually small. They are not always visible on ultrasound unless they are enlarged.
If you see lymph nodes, do not label them as malignant right away. Always correlate with clinical findings. Look for an underlying pathology that could explain the lymph node enlargement.
Mesenteric Adenitis Ultrasound
Mesenteric adenitis means inflammation of the mesenteric lymph nodes. On ultrasound, these lymph nodes appear enlarged.
When you see a cluster of three or more mesenteric lymph nodes in the right lower quadrant or the periumbilical region, and each node measures 8 mm or more in short axis, you can call it mesenteric adenitis.
The long axis of these nodes often measures more than 10 mm. However, the short axis measurement is more reliable when assessing for pathology.
Mesenteric adenitis is most commonly seen in children and young adults. It can mimic acute appendicitis because the pain is usually in the right lower quadrant.
There are two broad types of mesenteric adenitis:
- Primary mesenteric adenitis is diagnosed when enlarged lymph nodes are the only finding and there is no other identifiable inflammatory process in the abdomen.
- Secondary mesenteric adenitis occurs when the enlarged lymph nodes are associated with a detectable intra abdominal inflammatory condition.
It is frequently associated with upper respiratory tract infection.
In many cases, infected sputum is swallowed, which can lead to inflammation of the mesenteric lymph nodes.
Clinical Clues for Mesenteric Adenitis
- Mesenteric adenitis is most commonly seen in young males between 5 and 10 years of age. It is less common in females.
- Patients usually present with abdominal pain of longer duration rather than sudden onset.
- The pain is often located in the right lower quadrant and can closely mimic appendicitis. In some cases, the pain may be diffuse and involve the whole abdomen.
- Fever, general malaise, and loss of appetite are common associated symptoms.
- Nausea and vomiting may also be present.
- A recent history of sore throat, upper respiratory tract infection, or diarrhea is an important clinical clue and should always be asked during evaluation.
Ultrasound Features of Mesenteric Adenitis
- Size and Shape: The short axis diameter is 8 mm or more. This is the diagnostic threshold. The nodes are usually oval or round in shape.
- Location: There are usually multiple lymph nodes. You will often see three or more nodes clustered in the right lower quadrant.
- Echogenicity and Echotexture: The nodes are typically hypoechoic on ultrasound. In tuberculosis, you may see central necrosis within the node.
- Hilum: The hilum is an important feature. In viral or reactive cases, the hilum is usually preserved and remains visible. In bacterial infection or tuberculosis, the hilum may be effaced or lost.
- Color Doppler: On Doppler study, there is usually increased hilar vascularity.
- Associated Finding:
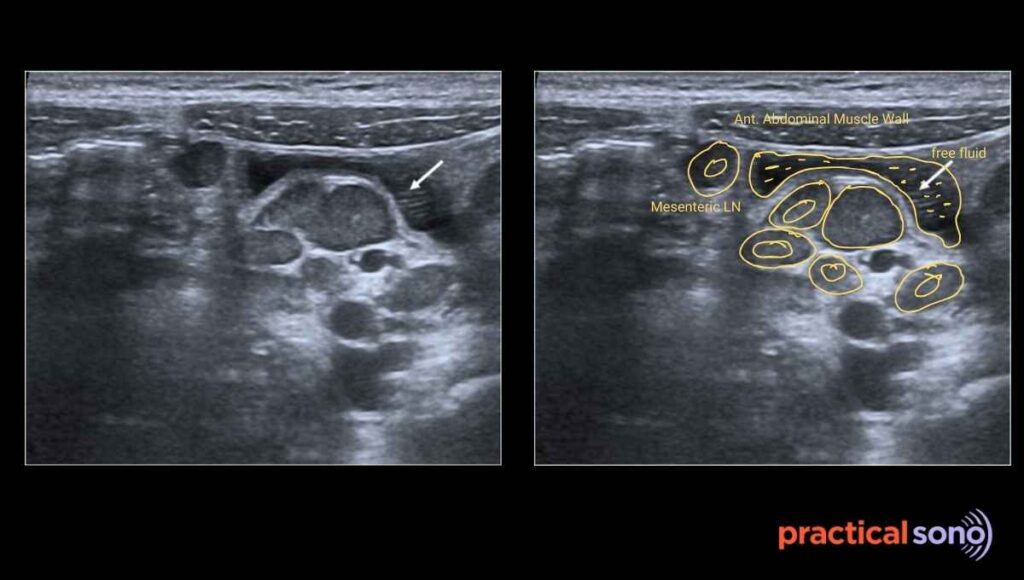
- The surrounding mesenteric fat may appear more echogenic due to inflammation.
- You may see a small amount of adjacent free fluid.
- The appendix appears normal. This is the key point that helps you differentiate mesenteric adenitis from acute appendicitis.
Reporting Mesenteric Lymphadenitis
Finding: Multiple enlarged mesenteric lymph nodes are noted in the right lower quadrant mesentery. The short-axis diameter of the largest node measures 10 mm. Nodes are oval, hypoechoic, with preserved hilum. Adjacent mesenteric fat appears mildly echogenic. A small amount of free fluid is present. The appendix is visualized and appears normal.
Impression: Sonographic features are consistent with mesenteric adenitis. No evidence of appendicitis.
Key Takeaway
Normal sized lymph nodes are usually not visible on ultrasound.
If you suspect mesenteric adenitis, carefully look for enlarged lymph nodes in the right iliac fossa and the periumbilical region.
Use the graded compression technique with a high frequency linear probe. This helps push bowel gas away and improves your view.
Always trace and document the appendix. This step is essential to rule out appendicitis.
Never assess lymph nodes in isolation. Always examine the bowel and the appendix. Look carefully for any associated bowel pathology.
Document the number of lymph nodes, their size, and their distribution.
If the hilum is preserved, the node is usually benign or reactive. If the hilum is lost or if there is necrosis, suspect tuberculosis or malignancy.
Mesenteric adenitis is usually self limiting. However, if the findings are persistent or atypical, investigate for secondary causes such as tuberculosis, lymphoma, or Crohn disease.
Remember the diagnostic criteria. There must be three or more lymph nodes in the right lower quadrant, and each must measure 8 mm or more in short axis, with a normal appendix.