These are common bowel pathology that can be diagnosed on ultrasound.
These pathologies are described based on simple practical framework. This will make it easy for you to approach and diagnose them.
We’ll describe each pathologies with this checklist in mind:
- Clinical clue ( Sign and symptoms, Investigation report)
- Is it large bowel or small bowel pathology?
- Wall thickness measurement
- Is it symmetrical or asymmetrical?
- Bowel diameter measurement
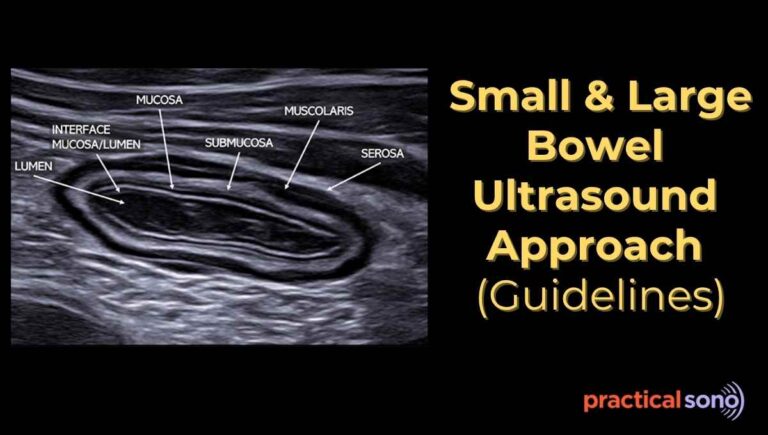
- Gut layers/ Gut signature
- Is it intact or disrupted?
- Peristalsis and luminal content
- Is it increased or decreased?
- Check the compressibility
- Is it compressible or not?
- Check vascularity
- Is it increased or absent?
- Look for associated finding (Secondary Sign)
- Inflammation of surrounding mesenteric fat (fat stranding)
- Fluid around lesion
- Free fluid in peritoneal cavity
- Air within wall
- Lymph node status
Common Bowel Pathologies Diagnosed on Ultrasound
#1 Appendicitis
- Clinical Clue: This is emergency condition, patient present with lower right abdomen pain, sudden begin at umbilicus then shifted. Ask patient to point the site of maximal tenderness. Put your probe there to look for dilated appendix.
- Wall Thickness: More than 3mm. Thickening is usually symmetrical in active inflammation but becomes asymmetrical in gangrenous or perforated appendicitis.
- Bowel Diameter: Outer-to-outer wall diameter exceeds 6 mm.
- Wall Stratification: In uncomplicated appendicitis, the normal “gut signature” is usually intact. A loss of stratification suggests advanced stages like gangrenous appendicitis or perforation.
- Bowel Peristalsis : Show no peristalsis.
- Vascularity: Color Doppler typically shows increased mural vascularity (hyperemia) in the appendiceal wall. Note that vascularity may decrease or disappear if the appendix becomes necrotic or gangrenous.
- Compressibility: The inflamed appendix is non-compressible under transducer pressure, maintaining its round shape.
- Luminal Content: The lumen may be distended with fluid hypoechoic or contain an appendicolith, an echogenic focus with posterior acoustic shadowing.
- Associated Finding: The appendix is identified as a blind-ending, tubular structure arising from the base of the cecum.
- Fat Stranding: Ultrasound shows increased echogenicity and prominent appearance of the periappendiceal fat, indicating inflammatory changes.
- Fluid around Lesion: A localized collection of free fluid around the appendix or in the right iliac fossa is a common secondary sign of inflammation or early perforation.
- Lymph Node Status: There may be enlarged reactive mesenteric lymph nodes (mesenteric lymphadenopathy) in the surrounding area
Learn more about Appendix Ultrasound.
#2 Intussusception
- Clinical Clue: Classically presents with a triad of intermittent colicky pain, a palpable “sausage-shaped” mass, and “currant jelly” stools, mostly in children. In children, intussusception is most commonly seen in the right upper quadrant, near the liver and kidney. Use these organs as sonographic landmarks.
- Wall Thickness: Appears as markedly thickened, multi-layered walls. This is actually a “wall-within-a-wall” appearance (the intussusceptum inside the intussuscipiens).
- Target / Doughnut Sign (Transverse View): Multiple concentric echogenic and hypoechoic rings represent the layers of the bowel wall. The central echogenic core contains mesenteric fat and vessels dragged into the intussusception. Pathologic intussusception usually has a diameter greater than 2.5 cm.
- Wall Stratification: Multiple concentric rings are visible. You will see the “Pseudokidney” sign in the longitudinal view, where the layers of the bowel mimic the appearance of a kidney.
- Pseudokidney / Sandwich Sign (Longitudinal View): The outer hypoechoic layer represents edematous bowel walls, and the central echogenic core represents mesenteric fat and vessels. It resembles the shape and texture of a kidney.
- Bowel Diameter: Significantly increased at the site of the lesion, often measuring 3–5 cm in total diameter.
- Bowel Peristalsis: Usually absent or diminished within the intussusception itself, though the bowel proximal to the site may show hyperperistalsis due to obstruction.
- Vascularity: Color Doppler is critical here. Preserved vascularity suggests the bowel is still viable; a lack of blood flow indicates ischemia or necrosis, making it a surgical emergency.
- Compressibility: The lesion is a firm, non-compressible mass.
- Luminal Content: The “inner” lumen may contain trapped fluid or mucosal echoes. You may also see a lead point (like a polyp, Meckel’s diverticulum, or enlarged lymph node) that triggered the telescoping.
- Associated Finding:
- The “Crescent in a Circle” sign, caused by mesenteric fat trapped between the layers of the bowel.
- Fat Stranding: Hyperechoic (bright) mesenteric fat is often seen pulled into the intussusception between the bowel layers.
- Fluid around Lesion: Peritoneal fluid (ascites) is common. If fluid is trapped between the telescoped layers, it significantly increases the risk of bowel failure.
- Lymph Node Status: Enlarged mesenteric lymph nodes are frequently found trapped within the layers (especially in “ileocolic” intussusception).
#3 Bowel Obstruction
- Clinical Clue: Patients usually present with abdominal distension, vomiting, and “tinkling” or absent bowel sounds.
- Wall Thickness: Initially normal or thinned due to stretching. If the obstruction is chronic or high-grade, the wall may become thickened (>3 mm) due to edema or ischemia.
- Visiblity of vavlulae connieventes as a stack of coin
- Wall Stratification: Usually intact early on. Loss of stratification is a “red flag” sign indicating bowel wall necrosis or impending perforation.
- Bowel Diameter: This is the primary diagnostic criteria. Small bowel loops are dilated >3 cm; the large bowel is dilated >5 cm.
- Fluid filled sausage shaped dilation of loops
- Bowel Peristalsis:
- Early/Dynamic phase: Hyperperistalsis (increased movement) as the bowel tries to push past the block.
- Late/Adynamic phase: Aperistalsis or “To-and-fro” movement (fluid moving back and forth without progressing).
- Vascularity: Variable. Increased mural blood flow (hyperemia) occurs with inflammation; absent flow on Color Doppler suggests strangulation (surgical emergency).
- Compressibility: Dilated loops are non-compressible and tense due to high intraluminal pressure.
- Luminal Content: Characterized by fluid-filled loops containing “whirling” echoes (the “Staircase sign”). In some cases, a “fecalization” appearance (fluid looking like solid stool) is seen.
- Associated Finding:
- The Transition Point—a sudden change from dilated, fluid-filled bowel to collapsed, empty bowel—which identifies the exact site of the blockage.
- Fat Stranding: Usually absent unless the obstruction is caused by an inflammatory process (like Crohn’s) or if the bowel is becoming ischemic.
- Fluid around Lesion: Free peritoneal fluid (ascites) between the dilated loops is a common finding (Tanga sign) and often correlates with the severity of the obstruction.
#4 Paralytic Ileus
- Clinical Clue: Unlike mechanical obstruction, this usually occurs after surgery (postoperative ileus) or due to electrolyte imbalances. Patients have a distended, “quiet” abdomen with absent bowel sounds.
- Wall Thickness: Typically normal or thin (<3 mm) because there is no primary inflammatory process or high-pressure blockage.
- Wall Stratification: Intact and well-preserved. Loss of layering is not expected in simple ileus.
- Bowel Diameter: Characterized by diffuse dilatation of both the small and large bowel. Loops are usually less distended than in mechanical obstruction, typically measuring 2.5–3 cm.
- Bowel Peristalsis: This is the defining feature. There is minimal to absent peristalsis (aperistalsis). Unlike mechanical obstruction, there is no “to-and-fro” motion; the fluid is static.
- Vascularity: Normal. Mural blood flow is usually preserved as there is no strangulation or mechanical tension on the vessels.
- Compressibility: The bowel loops are easily compressible because they are filled with gas or fluid without high-pressure resistance.
- Luminal Content: Predominantly gas-filled (showing “dirty” shadowing) or contains stagnant fluid. You won’t see the “whirling” fluid motion seen in mechanical blocks.
- Associated Finding:
- Lack of a transition point. There is no sudden change from dilated to collapsed bowel; the entire tract appears uniformly sluggish.
- Fat Stranding: Absent. The surrounding mesenteric fat appears normal.
- Fluid around Lesion: Usually absent. Significant free peritoneal fluid would suggest a different diagnosis (like peritonitis or perforation).
- Lymph Node Status: Normal (non-enlarged).
#5 Infectious Colitis
- Clinical Clue: Patients usually present with acute onset of bloody or watery diarrhea, fever, and diffuse abdominal cramping. On ultrasound, the “clue” is often pancolitis (involving the entire colon
- Wall Thickness: Characterized by mild to moderate circumferential thickening, more than 3mm. typically 4–8 mm. symmetrical.
- Wall Stratification: Generally intact and well-preserved. If stratification is lost, it suggests a more severe, necrotizing infection or progression to toxic megacolon.
- Bowel Diameter: The colon may be slightly narrowed due to wall edema or mildly dilated if the infection is causing secondary ileus.
- Bowel Peristalsis: Typically increased (hyperperistalsis) as the body attempts to expel the infectious contents, contributing to the patient’s diarrhea.
- Vascularity: Color Doppler shows increased mural blood flow (hyperemia), reflecting the active inflammatory response.
- Compressibility: The colon is usually compressible, though it may feel “stiff” compared to a healthy bowel due to the thickened walls.
- Luminal Content: Predominantly fluid-filled (hypoechoic) with little to no formed stool. You may see small echogenic debris reflecting mucus or inflammatory sloughing.
- Associated Finding:
- The “Haustral Fold” thickening—the characteristic folds of the colon appear prominent and swollen (the “accordion sign” on CT, seen similarly on US).
- Fat Stranding: Usually minimal to absent. Unlike diverticulitis or Crohn’s, infectious colitis typically doesn’t cause significant inflammation of the surrounding mesenteric fat.
- Fluid around Lesion: Small amounts of free peritoneal fluid (ascites) are common, especially in the paracolic gutters or the pelvis.
- Lymph Node Status: Often shows enlarged, reactive mesenteric lymph nodes (lymphadenitis), which are typically oval and have a preserved fatty hilum.
#6 Enteritis
- Clinical Clue: Patients usually present with periumbilical pain, nausea, and watery diarrhea. On ultrasound, the “clue” is seeing multiple hyperactive, fluid-filled small bowel loops, often in the mid-to-lower abdomen.
- Wall Thickness: Typically shows mild, symmetric thickening, usually ranging from 3–5 mm. ( > 3mm in distended bowel, .5mm in collapsed bowel)
- Wall Stratification: Almost always intact. The layers of the small bowel remain distinct despite the edema.
- Bowel Diameter: The loops are often mildly dilated (2–3 cm) because they are filled with fluid, but they do not reach the high-pressure distension seen in mechanical obstruction.
- Bowel Peristalsis: Classically increased (hyperperistalsis). You will see “rushing” fluid and rapid contractions as the small bowel tries to move contents along.
- Vascularity: Color Doppler shows mildly increased mural blood flow (hyperemia) due to the inflammatory response in the mucosa and submucosa.
- Compressibility: The loops remain easily compressible despite the wall thickening.
- Luminal Content: Entirely fluid-filled (hypoechoic) with floating echogenic “specks” representing digestive debris or mucus.
- Associated Finding:
- Prominent Valvulae Conniventes (the internal folds of the small bowel), which may appear slightly thickened or “fuzzy” on the screen.
- Fat Stranding: Usually absent. Significant fat inflammation is rare in simple infectious enteritis.
- Fluid around Lesion: It is very common to see small amounts of free fluid “triangles” tucked between the rounded loops of the small bowel.
- Lymph Node Status: Frequently associated with Mesenteric Adenitis—clusters of enlarged, oval, tender lymph nodes in the right lower quadrant or central mesentery.
#7 Ischemic Colitis
- Clinical Clue: Classically presents as an elderly patient with sudden onset of cramping left-sided abdominal pain followed by bloody diarrhea. On ultrasound, the “clue” is often localized thickening specifically at the splenic flexure or sigmoid colon (watershed areas).
- Wall Thickness: Characterized by moderate to marked circumferential thickening, often >5–9 mm, due to submucosal edema and hemorrhage. The bowel wall thickening is usually symmetrical and segmental, often involving long segments, and is most commonly seen in the left colon.
- Wall Stratification:
- Early/Reversible: Intact but with a very thick, hypoechoic submucosal layer (edema).
- Late/Infarction: Loss of stratification is a “red flag” indicating full-thickness necrosis.
- Bowel Diameter: The lumen is usually narrowed due to the massive inward swelling of the wall.
- Bowel Peristalsis: Characteristically absent or severely diminished (aperistalsis) in the affected segment.
- Vascularity: This is the most critical Doppler finding:
- Ischemic Phase: Absent or minimal mural blood flow (even with sensitive settings).
- Reperfusion Phase: May show hyperemia (intense flow) as blood returns to the injured tissue.
- Compressibility: The affected segment is rigid and non-compressible.
- Luminal Content: Often empty or containing a small amount of bloody fluid/debris.
- Associated Finding:
- The “Little Dot” sign—small bright echoes within the wall if air is starting to form (early pneumatosis).
- Pneumatosis Intestinalis (Air in the Wall): Appears as bright (echogenic) foci or linear streaks within the wall, often producing “dirty” shadowing. This is a critical finding that may indicate necrosis or transmural infarction.
- Fat Stranding: Usually mild to moderate. The surrounding fat may be hyperechoic, but typically less “angry” than in diverticulitis or Crohn’s.
- Fluid around Lesion: Free peritoneal fluid is common and, if echogenic (bloody), suggests a more severe grade of ischemia.
- Lymph Node Status: Usually normal. The absence of enlarged nodes helps differentiate ischemia from infectious colitis or malignancy.
- The “Little Dot” sign—small bright echoes within the wall if air is starting to form (early pneumatosis).
#8 Colon Cancer
- Clinical Clue: Patients often present with chronic symptoms like change in bowel habits, weight loss, or iron-deficiency anemia. On ultrasound, the classic “clue” is a focal, asymmetric mass that can be felt with the probe.
- Wall Thickness: Characterized by marked, irregular thickening, often >10–15 mm. It is usually eccentric (thicker on one side of the tube than the other).
- Wall Stratification: Almost always lost (disrupted). The cancer invades through the normal histological layers, destroying the “gut signature” and replacing it with a solid, hypoechoic mass.
- Bowel Diameter: The overall diameter of the segment may appear increased, but the luminal diameter is narrowed (stenosis), leading to the “apple-core” appearance.
- Bowel Peristalsis: The affected segment is rigid and aperistaltic. You may see hyperperistalsis in the healthy bowel segments proximal to the tumor if it’s causing an obstruction.
- Vascularity: Color Doppler typically shows disorganized, internal neovascularization (new blood vessel growth) within the tumor mass.
- Compressibility: The lesion is solid and non-compressible. It feels like a hard “lump” under the transducer.
- Luminal Content: Often shows a “Pseudokidney Sign”—the dark, thickened cancerous wall surrounds a bright, echogenic center (which is trapped gas or mucus in the narrowed lumen), mimicking the appearance of a kidney.
- Associated Finding:
- The “Shoulder Sign”—a sharp, abrupt transition where the normal bowel wall ends and the bulky, overhanging edges of the tumor begin.
- Fat Stranding: Often present and localized. If the cancer has breached the outer layer (serosa), the surrounding fat becomes hyperechoic (bright) due to desmoplastic reaction or direct invasion.
- Fluid around Lesion: Usually absent unless the tumor has caused a perforation or is associated with malignant ascites (peritoneal carcinomatosis).
- Lymph Node Status: Frequently shows enlarged, rounded, hypoechoic lymph nodes in the mesentery. Unlike reactive nodes, malignant nodes often lose their fatty hilum and appear “ink-spot” dark.
#9 Diverticulitis
- Clinical Clue: Classically presents as left lower quadrant pain (“left-sided appendicitis”) and fever. On ultrasound, the “clue” is point tenderness directly over a focal area of colonic wall thickening.
- Wall Thickness: Characterized by segmental, eccentric thickening (typically $>4$ mm). Unlike cancer, the thickening is usually more uniform along a short segment of the colon.
- Wall Stratification: Usually intact but may appear “fuzzy” due to edema. If a focal area shows a complete break in the wall layers, it suggests a micro-perforation or abscess formation.
- Bowel Diameter: The lumen is often narrowed due to the surrounding wall swelling and spasm.
- Bowel Peristalsis: The affected segment is aperistaltic and rigid.
- Vascularity: Color Doppler shows marked mural hyperemia (increased blood flow) in the thickened wall and the surrounding inflamed fat.
- Compressibility: The inflamed segment and the surrounding fat are non-compressible and very tender.
- Luminal Content: You may see the diverticulum itself—an out-pouching of the wall containing a bright, echogenic focus (fecalith) with “dirty” posterior shadowing from trapped air.
- Associated Finding: The “Dome Sign”—a small, rounded projection off the colon wall representing the inflamed diverticulum.
- Fat Stranding: Very prominent. This is a hallmark of diverticulitis; the surrounding mesenteric fat becomes hyperechoic (bright) and “creeping” around the colon, representing an intense inflammatory reaction.
- Fluid around Lesion: Often shows localized free fluid or a complex fluid collection (abscess) if the diverticulum has perforated.
- Lymph Node Status: Usually shows enlarged, reactive mesenteric lymph nodes in the immediate vicinity of the inflammation.
#10 Epiploic Appendagitis
- Clinical Clue: Presents as acute, localized pain (usually left or right lower quadrant) in a patient who otherwise looks well (no fever, normal labs). The “clue” is exquisite point tenderness directly over a fixed, fatty mass.
- Wall Thickness: Typically normal. A key differentiator from diverticulitis is that the adjacent colon wall is usually not thickened.
- Wall Stratification: Intact and completely normal, as the pathology is external to the bowel wall.
- Bowel Diameter: Normal. There is no narrowing or obstruction of the intestinal lumen.
- Bowel Peristalsis: Normal/Preserved. The bowel itself continues to move normally underneath the localized inflammation.
- Vascularity: Minimal to absent. The inflamed fat is often ischemic; however, you may see a “rim” of increased blood flow (hyperemia) in the surrounding tissues.
- Compressibility: The lesion itself is a firm, non-compressible oval mass.
- Luminal Content: Normal. Stool or gas is seen moving through the adjacent healthy bowel.
- Associated Finding: The “Hyper-echoic Nut”—an oval, fatty mass (typically 1–4 cm) attached to the serosal surface of the colon that does not move with respiration or pressure.
- Fat Stranding: Localized and intense. You will see a hyperechoic (bright) “halo” of inflamed fat immediately surrounding the infarcted epiploic appendage.
- Fluid around Lesion: Usually absent or minimal. If present, it is a very small, localized sliver of fluid near the mass.
- Lymph Node Status: Usually normal. The absence of lymphadenopathy helps distinguish this from more serious inflammatory or malignant conditions.
#11 Crohn’s Disease
- Clinical Clue: Patients often have a history of chronic diarrhea, weight loss, and recurrent abdominal pain. The ultrasound “clue” is often creeping fat and involvement of the terminal ileum (the most common site).
- Wall Thickness: Characterized by significant, often symmetric thickening, typically >4 mm and sometimes reaching 10–15 mm during acute flares.
- Wall Stratification:
- Early/Mild: Intact but with a thickened, hypoechoic submucosa (edema).
- Chronic/Severe: Loss of stratification (blurred layers) occurs due to deep ulcerations and transmural fibrosis.
- Bowel Diameter: The lumen is often narrowed (stenosis or “string sign”). You may see proximal dilation if a stricture is causing a partial obstruction.
- Bowel Peristalsis: The affected segments are rigid and aperistaltic (stiff-loop sign).
- Vascularity: Color Doppler shows marked mural hyperemia (increased blood flow). This is used clinically to distinguish an active inflammatory “flare” from chronic, inactive fibrosis.
- Compressibility: The bowel loops are firm and non-compressible.
- Luminal Content: Often shows fluid-filled narrowing or “star-shaped” patterns if the mucosal folds are severely ulcerated.
- Associated Finding: “Creeping Fat” (Fibrofatty Proliferation)—the mesenteric fat grows around the bowel loop, appearing as a thick, hyperechoic (bright) mass that displaces other bowel loops.
- Fat Stranding: Prominent and chronic. The fat appears “misty” or bright and is much more extensive than in simple infections.
- Fluid around Lesion: Free fluid is common. More importantly, ultrasound can detect fistulas (hypoechoic tracts between bowel loops) or abscesses (complex fluid collections).
- Lymph Node Status: Frequently shows multiple enlarged, oval, reactive mesenteric lymph nodes in the “basin” of the affected bowel segment.
Key Takeaway
This complete our 11 most common bowel pathologies that can be diagnosed on ultrasound. Remember, these are the common bowel pathologies that are frequently encounter during the clinical practice. This account for approx. 80-90% of bowel pathology seen on ultrasound. For other remaining rare type of pathologies, you need to recommend CR, MRI or biopsy.