Renal stone or calculi is common renal pathology that you’ll find during renal scan.
They are hard, solid, crystal-like masses. They appears echogenic foci within kidney urine collecting system- calyx, renal pelvis, and ureter.
Large stones can be easily seen. But, when it comes to small one, it becomes difficult to visualize them.
After reading this article, you will
- know types of renal stone and how they are formed
- understand the urine collecting system so that you know where to look for stone within kidney
- know the ultrasound features of renal stone
- find out how to correctly measure the renal stone
- also, know how to report your finding
Renal stone Overview
Types of renal stone
Based on chemical composition, there are four main types of renal stones.
- Calcium stone
- Uric acid stone
- Struvite stone
- Cystine stone
Calcium stones are the most common type.
Uric acid stones form when urine stays acidic for a long time. These stones are common in people with gout or diabetes. A diet high in animal protein also increases the risk.
Struvite stones are often called infection stones. They form due to urinary tract infections. The infection is caused by urea-splitting bacteria like Proteus or Klebsiella. These stones can grow very fast. They may form large staghorn calculi that fill the entire renal pelvis.
Cystine stones are rare and make up about 1 to 2 percent of cases.
Number of renal stones
Renal stones can be single or multiple.
About 63 percent of patients have a single stone at diagnosis. Solitary stones are the most common finding.
Multiple stones are less common. They often suggest an underlying metabolic disorder, such as hyperparathyroidism or renal tubular acidosis. Patients who have multiple stones at the start have a much higher risk of future stone episodes.
In some cases, multiple stones are present in both kidneys at the same time. This is seen in about 26 percent of cases.
Size of renal stone
Its size range from a grain of sand to a ping-pong ball. Stone size is measured in millimeters. It is the most important factor when deciding treatment.
5 millimeters. This is the number you have to remember.
Stones smaller than 5 mm have a high chance of passing on their own. Stones larger than 5 mm are less likely to pass spontaneously. These stones usually need medical expulsive therapy or surgical treatment.
Why?
The adult ureter has a very small internal diameter. It is usually only 3 to 4 mm wide. Because of this, 5 mm is a major clinical turning point.
Once a stone reach 5 mm or more, its size exceeds the natural elasticity of the ureter. This greatly increases the risk of obstruction.
PracticalSono Tips:
Stones smaller than 5 mm are difficult to see clearly on ultrasound. Ultrasound is very effective for stones larger than 5 mm, with sensitivity close to 100 percent.
For stones smaller than 5 mm, sensitivity is much lower. These stones may be missed completely. Studies show that about 70 to 75 percent of renal stone sized 3mm or less are not detected on ultrasound.
The classic ultrasound sign of a stone is an posterior acoustic shadow behind it.
Stones smaller than 5 mm often do not produce this shadow. This makes them hard to distinguish from bright kidney tissue or vascular calcifications.
Twinkling artifact:
Color Doppler may show a twinkling artifact that helps identify stones. However, this sign is also unreliable for stones under 5 mm. Its sensitivity is often very low.
When ultrasound does detect a small stone, it often overestimates the true size. Because of these limitations, current guidelines recommend a non-contrast CT scan when exact stone size and location are needed for treatment decisions.
Urine collecting system
The renal capsule is the outer covering of the kidney. It is a thin and fibrous layer of connective tissue.
On ultrasound, it appears as a thin, bright echogenic line. It forms a sharp and clear outer border of the renal parenchyma.
The capsule is very rigid. When the kidney becomes obstructed and swells, it cannot stretch. This is why obstruction causes severe pain.
Just beneath the capsule lies the renal cortex.
The cortex forms the outer part of the kidney tissue.
Renal columns are extensions of the cortex. They project inward and separate the renal pyramids of the medulla.
On ultrasound, the cortex looks smooth and uniform. It appears hypoechoic or isoechoic compared to the liver on the right and the spleen on the left.
Deep to the cortex is the renal medulla.
The medulla is made up of cone-shaped structures called renal pyramids. These pyramids are triangular or conical in shape.
They lie between the renal columns.
On ultrasound, the medulla is very dark. It is anechoic and is considered the most anechoic area in the abdomen.
At the center of the kidney is the renal sinus.
The renal sinus is a fat-filled cavity. Think of it as a room in the middle of the kidney.
It contains the renal pelvis, calyces, blood vessels, nerves, lymphatics, and fat.
On ultrasound, it appears as a bright central echogenic area. The large amount of fat and vessels makes it hyperechoic compared to the renal parenchyma. It is one of the brightest structures seen in the abdomen.
Renal calyces are cup-shaped structures. They collect urine from the renal pyramids. The minor calyces join together to form major calyces. These then come together to form the renal pelvis.
The renal pelvis is a funnel-shaped hollow structure. It collects urine from the calyces and directs it into the ureter. It is part of the urinary drainage system. Normally, it is collapsed and not visible on ultrasound. It becomes visible only when dilated.
The renal hilum is the concave area on the medial side of the kidney. This is where the renal pelvis, blood vessels, nerves, and lymphatic vessels enter and leave the kidney.
The ureters usually cannot be seen on ultrasound. They become visible only when they are dilated.
Understanding each of these structures clearly will help you read kidney ultrasounds with confidence.
Renal stones form when minerals in the urine become highly concentrated (and crystallize into solid particles. These crystals then aggregate and grow, often anchoring to the kidney tissue until they are large enough to obstruct the urinary tract.
Renal stones primarily form deep within the kidney, specifically on the renal papillae or within the collecting ducts and renal pelvis. Once they detach, they can migrate and lodge anywhere in the urinary tract, including the ureters, bladder, or urethra.
Fate of Renal Stone
The fate of a renal stone depends on its size, location, and movement.
One possible outcome is spontaneous passage.
Most small renal stones can pass out of the body naturally through urine.
About 80 to 90 percent of small stones pass on their own within a month.
Stone size plays a major role.
- 4 mm or less: These stone have about an 80 to 95% chance of passing naturally.
- 4 and 6 mm: 60 % chance of spontaneous passage. These stones often need medical expulsive therapy, such as Tamsulosin, to relax the ureter.
- Larger than 6 mm: Only about a 20 percent chance of passing. These stones often get stuck in ureter causing hydro nephrosis.
A stone may stay inside the kidney for many years without causing pain or damage. These stones are often found by chance during imaging done for other reasons.
There is a risk, though. About 70 percent of silent stones will grow or move.
This can later cause pain or complications.
The stone may also cause obstruction and other complications.
If a stone moves into the ureter but cannot pass, it can block urine flow.
This leads to hydronephrosis, where urine backs up and the kidney swells.
Pressure inside the kidney increases. Blocked urine can also cause infection.
This may lead to pyelonephritis or even life-threatening sepsis.
If obstruction lasts more than 2 to 4 weeks, permanent kidney damage can occur.
Recurrence is another important points to remember. Even after a stone is removed or passed, new stones can form. About 50 percent of patients will develop another stone within 5 to 10 years.
Clinical Clues of Renal Stone
- Abdominal pain: Most patients present with flank pain. The pain often radiates toward the groin or the genital region. This pain is usually colicky in nature. It comes in waves. The intensity increases and decreases as the ureter contracts to push the stone forward.
- Hematuria: It is a key diagnostic clue. Blood in urine is seen in about 85 to 90 percent of symptomatic patients. Patients may also complain of urinary urgency and increased frequency.
- Nausea and vomiting: It is extremely common. These happen as a reflex response to severe renal colic.
- Fever and chills are very important warning signs. Their presence suggests an infected stone. This condition is called obstructive pyelonephritis and requires urgent attention.
Ultrasound Features of Renal Stone
While doing scan in patient with above clinical features, always ask yourself a few questions.
- Is there a stone present?
- Where exactly is the stone located?
- How large is the stone?
- Is the stone causing obstruction?
Is there a stone present?
The first step is to identify the stone in the kidney.
Renal stones form only in the urine collecting system. They are not found in the renal cortex or the medulla. Scan from the calyces to the renal pelvis and down toward the urinary bladder.
Look for bright structure in these region.
On ultrasound, a stone appears as a hyperechoic focus.
This means it looks very bright or white. It is much brighter than the surrounding kidney tissue.
Another important feature is posterior acoustic shadowing.
Stones are dense, so they block ultrasound waves.
This creates a dark shadow just behind the stone.
Large stones, usually more than 5 mm, produce a clear and strong shadow. Small stones, less than 5 mm, may not show a shadow.
These small stones can be confused with renal fat or calcified blood vessels. Because small stone does not produce shadow, they are very difficult to find, especially when present in renal sinus which is also hyperechoic.
In this scenario, Color Doppler can help.
When Doppler is turned on, the stone may show rapid red and blue color changes behind it.
This looks like turbulent blood flow, but it is not true flow. This is called twinkling artifact.
This sign is very helpful.
It is often more sensitive than shadowing, especially for small stones.
Twinkling happens because ultrasound waves interact with the rough surface of the stone.
Scan the kidney in both longitudinal and transverse views. Slowly sweep through the entire kidney. This is very important so you do not miss any additional renal stones. Note down the number of stone you see.
Where exactly is the stone located?
The kidney is universally divided into these three distinct anatomical regions or “poles.”
- upper pole
- mid pole
- lower pole
The upper pole, also called the superior pole, is oriented toward the patient’s head. On the right side, it lies close to the upper part of the liver. On the left side, it sits beneath the spleen.
The mid-pole, or interpolar region, is the central part of the kidney. This is where the renal artery and vein enter and the renal pelvis exits. It is the thickest portion of the kidney, and the renal sinus appears as a bright white center here.
The lower pole, or inferior pole, is oriented toward the patient’s feet.
Stones in the lower pole are the most difficult to pass. Because they sit at the “bottom of the bag,” they have to travel uphill against gravity to get out of the kidney.
If the stone has moved out of the kidney and into the ureter, record its location based on how far it is from the bladder and kidney. However, for surgical planning, the bladder is often used as the primary reference point.
How large is the stone?
Always measure the stone in both the longitudinal and transverse views. The reported stone size is the maximum diameter seen in any view.
- Place the calipers on the greatest linear distance between the two bright, hyperechoic edges of the stone.
- For the most accurate measurement, turn on tissue harmonic imaging. This improves lateral resolution and makes the stone borders sharper and clearer.
- Also adjust the focal zone. Place the focus at or just in front of the stone. This gives you the sharpest edges for correct caliper placement.
- Next, adjust depth and gain.
- Reduce the gain slightly. Too much gain causes the bright stone surface to spread into nearby tissue. This can make the stone look larger than it really is and leads to overestimation.
Remember, ultrasound often overestimates stone size by about two to three millimeters.
Is the stone causing obstruction?
Next, look carefully for complications.
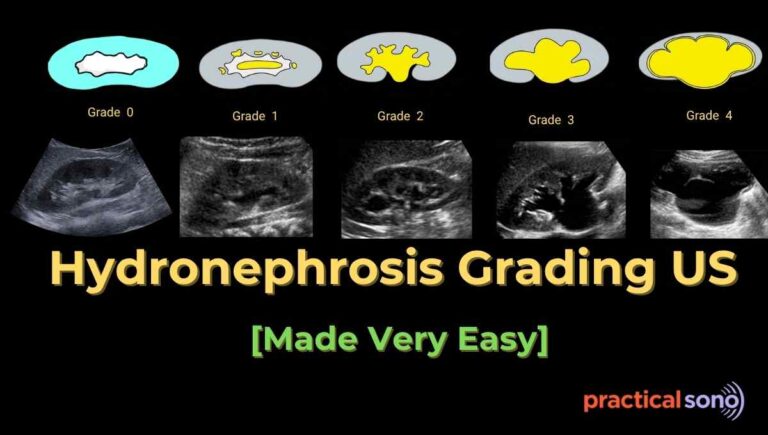
The most common complication is hydronephrosis. It is dilation of entire collecting system of urine. This includes both the renal pelvis and the calyces.
Calectasis means dilation of the calyces only. It refers to widening of the individual calyces, which look like fingers of the drainage system.
If a report mentions isolated calectasis, the stone is usually small or only partially blocking one branch of the kidney. If a report mentions gross hydronephrosis, this suggests a major obstruction, most often in the ureter. This situation needs urgent medical attention to protect kidney function.
If hydronephrosis is present, calectasis is almost always part of it.
Reporting Renal Stone
Here are some tips while reporting the renal stone:
Laterality : Always mention the side. Say right kidney, left kidney, or bilateral. Never write “renal calculus seen” without specifying the side.
Location: Always report the exact location of the stone. This can be the renal pelvis, upper pole, mid pole, lower pole, or pelvi-ureteric junction (PUJ). Example: “Echogenic focus noted in the lower pole of the right kidney.”
Number of Stones: Specify if it is single or multiple. Example: “Single calculus” or “Multiple calculi, largest measuring …”
Size: Measure the stone in millimeters. Use the plane where it looks largest. Measure outer-to-outer margins, not the shadow. Example: “Measures 6 mm in maximum diameter.”
Acoustic Shadow: Note if there is posterior acoustic shadowing. Example: “Shows posterior acoustic shadowing.”
If no shadow, say: “No definite posterior shadow seen, likely small calculus.”
Twinkle Artifact: If you use color Doppler, mention twinkle artifact. Example: “Color Doppler shows twinkle artifact at the site of calculus.” This helps confirm small stones.
Obstruction Assessment: This is very important. Check the pelvicalyceal system for hydronephrosis. Mention its grade. Mild, moderate, or severe. Example: “Mild dilatation of pelvicalyceal system noted.
Renal Size and Parenchyma: Always comment on kidney size, cortical echogenicity, and thickness. Chronic obstruction can cause thinning and kidney damage.
Limitations: Always mention limitations. Example: “Distal ureter not visualized due to bowel gas.” Or “Small ureteric calculi may be missed on ultrasound.”
Sample Standard Ultrasound Report
Findings:
Right kidney measures 10.5cm x 5 cm with normal cortical echogenicity and preserved corticomedullary differentiation. A 6 mm echogenic focus with posterior acoustic shadowing is seen in the lower pole of the right kidney. Mild pelvicalyceal dilatation noted. No perinephric collection. Left kidney normal. Urinary bladder normal.
Impression:
Right lower pole calculus measuring 6 mm with mild hydronephrosis. Suggests partial obstruction. Clinical correlation advised.
Optional Recommendations:
Add only if relevant: hydronephrosis present, stone larger than 5–7 mm, or severe symptoms. Example: “Correlation with clinical findings and renal function tests advised. Non-contrast CT KUB may be considered if clinically indicated.”
Renal Stone vs Renal Concretion
Confusion between renal stone and renal concretion is extremely common.
A renal concretion is a broad medical term. It means any hardened or calcified mineral deposit inside the kidney. This term is often used in imaging reports, especially ultrasound. It usually describes very small or early deposits. These deposits have not yet become true stones or caused symptoms.
A renal stone, also called a calculus, refers to a fully formed crystalline mass. It develops through the process of urolithiasis. These stones are more solid, better defined, and more likely to cause pain or obstruction.
Understanding the difference helps you describe ultrasound findings more accurately and guides proper patient management.
Key Takeaway
Renal stone are common ultrasound finding during renal scan. Large stone are easy to see. However, small stone less than 5mm are much difficult to visualize. In such case, knowledge about urine collecting system and use of color doppler for showing twinkling artifact can immensely help.
Always, rule out the hydro nephrosis while assessing the renal stone.